Introduction: Despite the limited pieces of evidence on the cardiovascular safety of testosterone replacement therapy (TRT) in men with late-onset hypogonadism (LOH) and functional hypogonadism (FH), its global use for hypogonadism management is surging. This review aims to determine TRT's long-term safety.
Methods: A systematic review was conducted using the preferred reporting items for systematic reviews and meta-analyses (PRISMA) 2020 guidelines. Six databases (PubMed, Scopus, Wiley Library, Embase, Cochrane database for systematic reviews and Google Scholar) were searched for relevant articles. The Distiller-SR software was used for journal screening, duplicate removal and data extraction.
Results: This review included 23 eligible publications (10 RCTs and 13 cohort studies) involving 102,139 participants. Although only seven studies reported major adverse cardiovascular events (MACE) outcomes, many others examined cardiovascular risk factor benefits and or adverse effects.
Conclusion: Long-term use of TRT in men with LOH and FH appears to offer cardiovascular benefits, provided safe practices are followed. However, caution is advised on the use of TRT in hypogonadal men with pre-existing cardiovascular disease.
Testosterone replacement therapy, Cardiovascular outcome, Late-onset hypogonadism, Functional hypogonadism, Cardiovascular safety
Testosterone plays a significant role in the growth and maturation of secondary sexual characteristics, and the development of sexual and cognitive functions [1]. However, these functions could be impaired by the insufficient production of testosterone from the testes with or without affectation of the hypothalamus-pituitary axis and that is known as male hypogonadism [2]. Male hypogonadism may present with non-specific symptoms and signs such as decreased energy, poor concentration, sleep disturbance, and depressed mood to specific clinical features such as incomplete or delayed sexual development, low libido, small testes, loss of axillary and pubic hair [3]. Overall, hypogonadism has a prevalence rate of 2.1% and this increases with age, peaking at about 5.1% in men over 70 years [4,5].
Hypogonadism can also be classified into organic or functional hypogonadism (FH). Organic hypogonadism, also known as classical or pathological hypogonadism results from medical conditions affecting the hypothalamic-pituitary-gonadal (HPG) axis, leading to a deficiency of androgen. Organic hypogonadism can be further classified into primary (hypergonadotropic hypogonadism) or secondary (hypogonadotropic hypogonadism). Whereas, FH can occur in the setting of an intact HPG axis [3]. This is common among men with Obesity, (T2DM), medical co-morbid conditions (such as heart, liver and kidney failures), people using opioids, glucocorticoids and anabolic steroids and those who engage in excessive exercise. Functional hypogonadism is a diagnosis of exclusion as there are clinical features in keeping with androgen deficiency, absence of structural HPT axis pathology without specific pathologies suppressing the HPG axis, in the presence of low serum testosterone [6].
Hypogonadism attributed to advancing age was previously referenced by many names including partial androgen deficiency in ageing males (PADAM), and testosterone deficiency syndrome (TDS), amongst others. However, in recent times, this condition is generally referred to as Andropause or late-onset hypogonadism (LOH) [7]. Late-onset hypogonadism is defined as subnormal or low serum testosterone levels with an array of physical, psychic, and sexual symptoms generally related to male hypogonadism [8]. There is evidence of a decline in testosterone production with advancing age, especially after 40. The mean decline in serum testosterone levels is about 1% per year between ages 40 and 70. Some of the mechanisms identified to be responsible for LOH and FH include atherosclerosis-related reduction in the activity and amount of Leydig cells with a decrease in the amplitude and frequency of luteinizing hormone (LH) because of dysregulation of the hypothalamic pulse generator. Apart from testosterone, other hormones like insulin-like growth factors, thyroid hormones, cortisol, etc also decline in ageing men [8].
Over the years, cardiovascular diseases have remained a leading cause of morbidity and mortality worldwide, with men having higher mortality than women. This increased risk in men is assumed to be due to the presence of androgens [9]. Low circulating endogenous testosterone has been associated with several CV adverse effects such as endothelial dysfunction, central adiposity, and diabetes mellitus (DM) [10]. CV events are reduced in men with upper normal values of endogenous testosterone levels compared with men with low circulating testosterone [11].
The Endocrine Society recommends that male hypogonadism should be treated with testosterone replacement therapy (TRT) to correct symptoms of androgen deficiency and to induce or maintain sexual functions. TRT was approved for the treatment of male hypogonadism in 1972 by the United States Food and Drug Administration (FDA) to alleviate symptoms and improve quality of life [12]. It is the only evidence-based treatment for LOH and cases of functional hypogonadism that are not reversible after the underlying aetiology has been removed underlying aetiology [13]. Although, Hypogonadal men on TRT who achieved a mid-normal range of serum testosterone have improved CV risk factors, those over or under-treated with TRT have an increased risk of CV events [11]. Concerns exist about the CV safety of TRT in men with androgen deficiency due to higher testosterone levels linked to increased risk of prostatic enlargement, cancer, and polycythaemia [12].
However, no significant links between TRT and major adverse cardiovascular events such as MI, stroke, or heart failure hospitalization have been documented [14]. This review aims to evaluate TRT's long-term CV safety and provide a protocol for monitoring its efficacy and safety in men with LOH and FH.
This systematic review was approved by the University of South Wales Ethics Committee. The project proposal was also registered with the International Prospective Register of Systematic Reviews (PROSPERO) and the title of the systematic review was registered on the 16 th of April 2022 with the registration number - (CRD 42022314247). The Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) 2020 set of standards checklists were followed in conducting this work [15]. Below are the inclusion and exclusion criteria for the study participants.
1. Randomized controlled trials as well as observational studies evaluated the impact of long-term TRT use on CV risk in men with late-onset hypogonadism.
2. Trials on FH that include obesity, drug-induced testosterone deficiency (e.g., gonadotrophin-releasing hormone agonist or antagonist, and chronic opioid use or abuse) and co-morbid medical illnesses such as DM, chronic obstructive pulmonary disease, and human immunodeficiency virus-associated weight loss.
3. Studies that made use of TRT for the long-term (twelve months or more) as well as determining the CV safety or adverse profile of TRT.
1. Studies that do not examine or access the CV risk or safety of TRT.
2. Studies, where TRT was not used for up to twelve months, will be excluded. It will be difficult to access long-term CV risk and safety in studies that made use of TRT within a brief period [12].
3. Trials that made use of other forms of testosterone formulations or adjuvants such as selective androgen receptor modulators (SARM) or selective oestrogen receptor modulators (SERM).
4. Studies that involved transgender individuals that used TRT.
We searched six databases, including PubMed, Scopus, Wiley Library, Embase, Cochrane Database of Systematic Reviews, and Google Scholar. The search covered published journals or manuscripts on LOH and FH from inception to March 31, 2022. The lead reviewer conducted and designed the search for each database, with input from two other reviewers. The following keyword combinations were used: LOH and TRT, LOH with cardiovascular risk or safety, LOH and TRT with cardiovascular risk/safety, FH and TRT, FH and cardiovascular risk/safety, and FH with TRT with cardiovascular risk/safety. Abstracts meeting the inclusion criteria underwent further searches for full manuscripts. Mendeley's reference manager aided in obtaining journal articles and references.
All articles found were uploaded to Distiller SR software from the Mendeley reference manager and duplicates were removed to a separate folder. Journal titles and abstracts were screened for eligibility using standardized instructions by two independent reviewers. Eligibility criteria were iterated for consistency and clarity to aid calibration between reviewers right from the screening of eligible titles or abstracts to the data extraction phase. Any missing articles were obtained through other means, such as the University of South Wales Library and Research Gate. Disagreements were resolved by the third reviewer or by consensus among the three reviewers.
The full-text journal articles meeting the eligibility criteria were automatically transferred to the next review phase, which is data extraction in the web-based collection form of Distiller SR. The study characteristics such as population, mean age with standard deviation, gender, inclusion and exclusion criteria, numbers randomized, numbers treated, study design (randomized controlled trials or cohort studies), study location, period, follow-up value and measure, method of randomization, treatment received, study limitations and conclusions were extracted. The data of interest included long-term cardiovascular safety of TRT among people with LOH and FH, doses, and frequency of TRT leading to cardiovascular adverse outcomes, especially MACE outcomes such as acute MI or ischemia, stroke, and heart failure. Two reviewers independently extracted the data, and any conflicts were resolved by the third reviewer according to the study's objectives and eligibility criteria.
When conducting a systematic review, publication, citation, and dissemination biases commonly occur. To mitigate these biases, only articles that met the eligibility criteria were included [16].
This systematic review focused on two primary outcome measures: the long-term cardiovascular safety of TRT (12 months or more) and the incidence of MACEs, including MI, stroke, heart failure, and all-cause mortality.
The objective of this study was to evaluate available data on the long-term cardiovascular safety of TRT, utilizing various study designs. Descriptive statistics, such as mean, median, percentages, and standard deviation, were employed to synthesize the findings.
A search of multiple databases yielded a total of 7,966 journal article titles and abstracts, including Pubmed (2317), Scopus (1563), Cochrane Library (10), Embase (2338), Google Scholar (1372), and Wiley Library (366). After removing duplicates and applying eligibility criteria, 782 journal titles and abstracts were included in the secondary screening level. Following further duplicate removal, 117 articles were reviewed in full text, resulting in the identification of 23 publications meeting the inclusion and exclusion criteria. There was moderate agreement between reviewers (kappa (k) = 0.40). Figure 1 provides a linear algorithm of the search strategy that yielded 23 RCTs and observational studies using TRT in men with LOH and FH for 12 months or more.
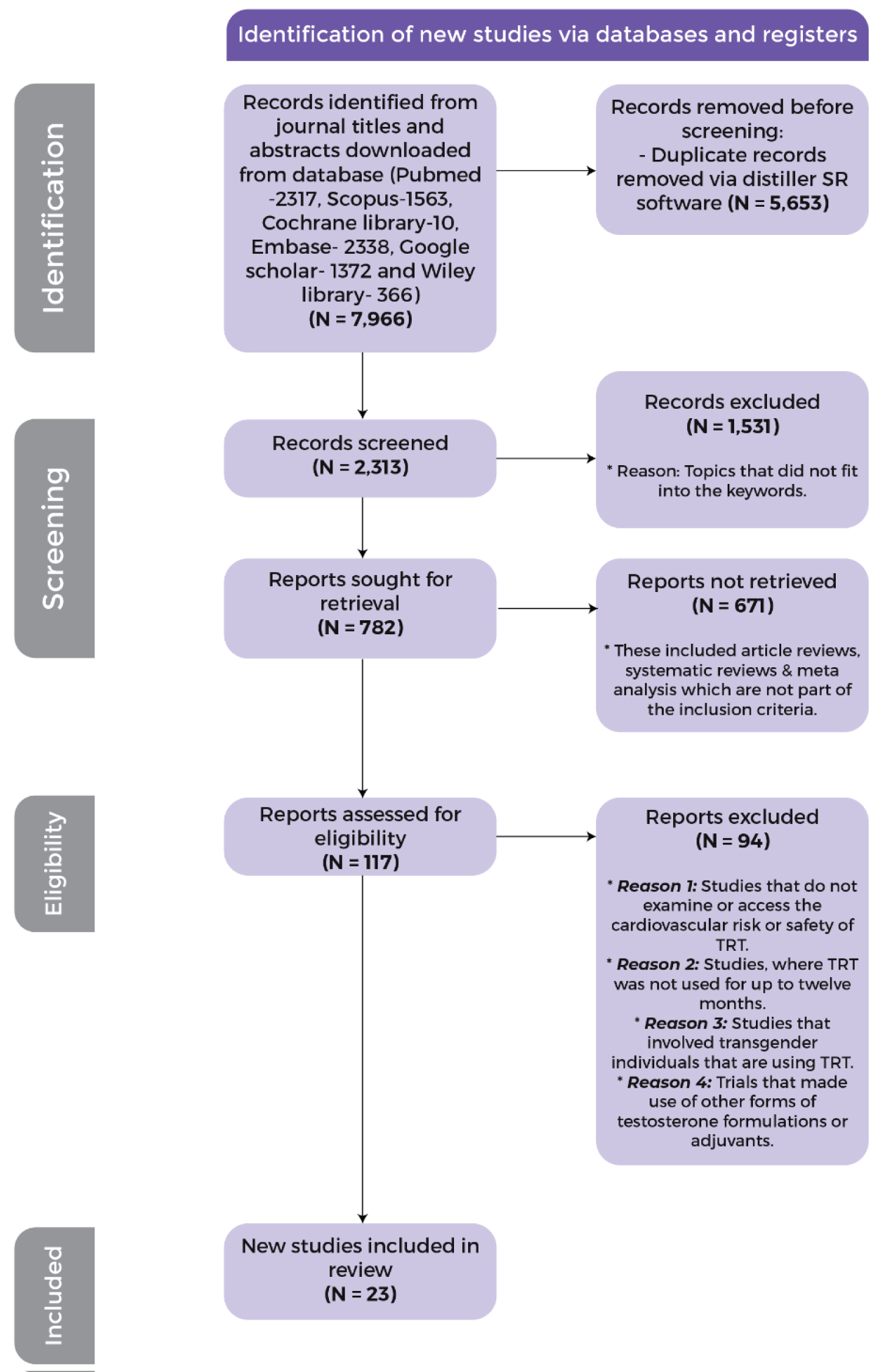 Figure 1: Search strategy resulting in 23 randomised control trial and observational cohort studies.
View Figure 1
Figure 1: Search strategy resulting in 23 randomised control trial and observational cohort studies.
View Figure 1
Table 1 presents the 23 publications, which included a total of 102,139 participants in 10 RCTs and 13 observational studies, both prospective and retrospective, with varying durations over 12 months, the longest being eight years. The age range of participants was middle-aged and older.
Table 1: Characteristics of included studies. View Table 1
Only seven of the included studies reported MACE as an outcome measure, while 19 studies reported measures on CV risk factors' benefits and/or adverse effects (Table 2), and eight studies commented on all-cause mortality.
Table 2: Characteristics of inventions, cardiovascular risks and/or events of included studies. View Table 2
TRT has beneficial effects in hypogonadal men, improving symptoms and sexual performance. However, long-term TRT use in older men with CVD may increase cardiovascular events. This review focuses on studies of TRT use for a year or more in LOH/FH men and its impact on CV outcomes.
In their 2018 study, Groti, et al. [17] examined the impact of testosterone replacement therapy (TRT) on metabolic syndrome and vascular functions in 55 hypogonadal, obese men with type 2 diabetes over 12 months. The participants were divided into two groups: The first group, which consisted of 28 individuals, received testosterone undecanoate injections (1000 mg IM every 10 weeks), while the second group was given a placebo. The results of the study indicated that the testosterone group showed a significant improvement in flow-mediated dilatation (P = 0.005) after one year of TRT, while the placebo group showed no change (P = 0.94). Moreover, the decrease in intima-media thickness (IMT) was twice as significant in the testosterone group compared to the placebo group (P < 0.001 and P = 0.006, respectively). The study also revealed that TRT decreased waist circumference (WC), body mass index (BMI), total cholesterol, and endothelial dysfunction, while improving insulin sensitivity and glycaemic control in obese, hypogonadal men with T2DM.
In the BLAST (Birmingham, Lichfield, Atherstone, Sutton, Coldfield, and Tamworth) study [18], TRT was administered for over a year. The study included a 30-week RCT multicentre trial, followed by a 52-week open-label phase, with the primary goal of assessing the effects of long-acting testosterone undecanoate on sexual function, mood, and quality of life, without considering MACEs. The study discovered that low testosterone levels were associated with CV risk factors such as impaired glycaemic control, higher BMI, increased severity of erectile dysfunction, and WC. Additionally, long-term use of TRT resulted in a substantial reduction in HbA1c as early as six weeks, with the reduction persisting for 82 weeks.
Similarly, in 2014, Hackett, et al. [19] evaluated the changes in HbA1c and serum testosterone levels necessary for response in hypogonadal men with T2DM. HbAIc significantly reduced by 0.41% within six weeks and dripped further by 0.46% after 52 weeks of open-label use. Furthermore, insulin sensitivity improved, alongside a significant decrease in weight, BMI, and WC for up to 82 weeks in T2DM hypogonadal men without depression who achieved adequate serum testosterone levels following TRT long-term use. There was no substantial increase in CV events.
Hackett and his colleagues in 2019 conducted a double-blind randomized placebo-controlled study to determine the effect of TRT on mortality in T2DM men with hypogonadism and to assess whether discontinuation of TRT would increase mortality [20]. The study followed 857 men with T2DM for over 3.8 years, stratifying them based on testosterone levels into two groups: Those with normal testosterone and those with hypogonadism. The hypogonadal group was further subdivided into those on TRT and those not on TRT, with the TRT group being further subdivided into those whose TRT was continued and those whose TRT was discontinued. At baseline, men with normal testosterone levels had lower blood pressure, BMI, HbA1c, and triglycerides and higher HDL compared to hypogonadal men, indicating that male hypogonadism is a cardiovascular risk factor. The study found no significant improvement in cardiovascular risk factors among those with normal testosterone levels or those on TRT after 3.8 years of follow-up, except for waist circumference. However, there was a reduction in mortality among men with normal testosterone levels and those with hypogonadism on TRT, particularly in older men with lower weight (< 93.8 kg).
The study's limitations include the exclusion of MACE from the primary objective, the wide age range of participants (18 to 80 years), and only 78 hypogonadal men on TRT out of 175 completing the study without discontinuing TRT. In conclusion, the BLAST study publications [18-20] demonstrate that the use of TRT results in sustained improvement in cardio metabolic risk factors over a prolonged period and has a greater impact on older men with lower weight in reducing mortality.
In a BLAST follow-up study, published in 2020, it was observed that there was an improvement in erectile function with long-term TRT use in T2DM hypogonadal men, but the benefit diminished upon discontinuation [21]. TRT also reduced visceral fat and did not affect non-fatal MACE when untreated T2DM hypogonadal men were compared (19.8/1,000 years) to treated T2DM hypogonadal men (15.2/1,000 years) with TRT.
The Times2 study [22] was a 12-month multicentre RCT that evaluated a novel transdermal 2% testosterone gel on CV risk factors, insulin resistance, and symptoms of 220 hypogonadal men with T2DM and/or metabolic syndrome. TRT reduced homeostasis model assessment of insulin resistance (HOMA-IR) by 15.2% (95% CI 3-26, P = 0.018) compared to placebo at 6 months and 16.4% at 12 months (P = 0.006). Glycaemic control was significantly better than placebo at 9 months with an HbA1c difference of -0.446% (P = 0.035). TRT also improved lipid parameters, particularly in the metabolic syndrome subgroup, lipoprotein little a (Lpa), low-density lipoprotein (LDL), total cholesterol and increased libido. TRT reduced Lpa by -0.235 µmol/L (CI -0.431 to -0.039, P = 0.019) in the overall intention-to-treat group, a strong independent CV risk factor for premature coronary artery disease. HDL decreased significantly in the TRT group compared to placebo by -0.049 mmol/L (CI -0.094 to -0.004, P = 0.032). No significant effects on body fat, BMI, WC, triglycerides, and sexual satisfaction. Cardiovascular events were more common in the placebo group (10.7% vs. 4.6%, P = 0.095), but not an outcome measure. Long-term TRT was shown to improve metabolic profiles without worsening CV risk in hypogonadal men with T2DM and metabolic syndrome.
A single-blinded RCT was conducted to assess the effects of 52 weeks of supervised exercise and diets, with or without TRT (transdermal testosterone), on glycaemic control and metabolic syndrome components in hypogonadal men with metabolic syndrome and newly diagnosed T2DM [23]. Both groups showed improvement in metabolic indices, lipids, and serum testosterone after 52 weeks of treatment. However, the addition of topical testosterone (50 mg of testogel, once daily) significantly improved all parameters compared to the diet and exercise alone group. Thus, supervised dietary management and exercise with topical testosterone supplementation are beneficial for hypogonadal men with T2DM in achieving glycaemic and metabolic targets. The study did not measure major adverse cardiovascular events.
Francomano and his team conducted a prospective cohort study in Rome, Italy to investigate the effects of long-term TRT on metabolic and hormonal profiles of Forty hypogonadal men with metabolic syndrome [24]. Twenty participants for whom testosterone was contraindicated served as controls while the remaining twenty participants received IM testosterone undecanoate every 12 weeks for 60 months, In comparison to controls, the test group showed significant improvements in body weight, WC, blood pressure, HbA1c, insulin sensitivity, total cholesterol/HDL ratio, femoral neck and lumbar T scores, as well as hormonal profiles (serum vitamin D, thyroid-stimulating hormone, insulin-like growth factor-1, and growth hormone). TRT long-term use was shown to improve CV risk factors such as anthropometric, metabolic, and hormonal profiles of hypogonadal men with metabolic syndrome.
In a double-blinded RCT study with follow-up by Groti, et al. [25], evaluating TRT effects effect on glycaemic control, insulin resistance, lipids, visceral obesity, endothelial dysfunction (via FMD), and Carotid artery morphology (via IMT) in hypogonadal obese men with T2DM. The test group (28 individuals received IM testosterone undecanoate for 2 years) while the control group initially received a placebo before switching to IM testosterone in the second year. TRT use improved glycaemic control (FPG, HbA1c), HOMA-IR and IMT. Additionally, lipid profile improved alongside FMD, serum testosterone levels, and sexual function (although not statistically significant) in comparison to controls. Another similar research done on TRT safety in obese males with FH and T2DM showed the same findings [26]. Thus, it can be inferred from both studies, that long-term use of TRT in T2DM men with high-risk obesity and FH is safe with significant improvement in CV risk factors.
Francomano, et al. [27] conducted an open-label parallel-arm observational study to investigate TRT effects on cardiovascular and metabolic profiles in obese hypogonadal men and the durability of improvements after withdrawal. The study involved 24 severely obese hypogonadal men, with 12 assigned to receive IM testosterone every 12 weeks for 54 weeks in addition to diet and physical exercise (DPE), while the other 12 received DPE only. After 54 weeks, participants underwent a 24-week testosterone withdrawal phase. Results showed that the group receiving DPE plus testosterone had significant improvements in several parameters including ejection fraction, diastolic function, carotid intima-media thickness, and endothelial function (p < 0.01). Insulin sensitivity, total cholesterol, fibrinogen, microalbuminuria, and hormonal profile also improved. However, after 24 weeks of testosterone withdrawal, all cardiac and hormonal parameters returned to baseline except for body fat and blood pressure.
Haider and his cohort investigated the benefits of restoring serum testosterone to optimal levels in obese hypogonadal men regarding weight loss and metabolic profile [28]. The study involved 181 hypogonadal obese men with cardiovascular (CV) risks, who received 1000 mg of IM testosterone injection every 12 weeks for 60 months. Results showed significant improvements in weight, waist circumference, BMI, serum glucose, lipid parameters, and blood pressure readings of all participants, particularly those with type 2 diabetes mellitus, compared to baseline and each subsequent year. The findings suggest that TRT can improve the CV risk and metabolic profiles of obese hypogonadal men with CV risk factors.
Alwani, et al., [29] studied TRT’s long-term effects on hypogonadism and erectile dysfunction (ED) in men with a history of CVD The study involved 77 men with FH and ED who received IM testosterone undecanoate every 12 weeks for eight years after excluding those without CVD. Results showed a significant decrease in weight, systolic blood pressure, HbA1c, and total cholesterol, with an increase in HDL-C. There was also a significant improvement in the international index of the erectile function domain. These suggest that TRT long-term use provides vascular benefits, protection against CV events, and improved erectile function in men with FH.
A group of researchers led by Al-Qudimat assessed the association of long-term TRT use over 8 years in 496 hypogonadal men with non-alcoholic fatty liver disease, hepatic steatosis, and CVD [30]. They found a significant reduction in WC, BMI, fatty liver index, and serum triglycerides in the testosterone group compared to the control (those who opted out). The testosterone group had 25 deaths (8.0%), of which 11 were attributed to CVD, while the control group had 28 deaths, all related to CVD (P = 0.035). The study suggests that long-term TRT use benefits liver function and reduces the CV-related mortality of hypogonadal men with hepatic steatosis. However, 140 out of 312 participants in the testosterone group discontinued their treatment after 5.5 years of using TRT for about 17 months before recommencing, which is a limitation of this study.
The Registry of Hypogonadism in Men (RHYME study) was a multinational registry of men with hypogonadism in six European countries that assessed the long-term cardiovascular safety of TRT for up to three years [31]. Out of 999 eligible participants, 750 were assigned to testosterone therapy, with 70.5% consistently using TRT. Administered testosterone prescriptions include topical gels (68%), injectable testosterone (31%) and oral testosterone (2%). CV events occurred in 41 participants, with similar frequency in both groups. There was no significant difference in the overall incidence of CV events between TRT-treated and untreated men, and no increased CV risk in this large and diverse cohort of hypogonadal men regardless of TRT type (1697.4 vs. 1480.0 per 100,000 person-years = 0.7). Advancing age and prior history of CVD, but not TRT were significant predictors of new-onset CV events or outcomes. The study concluded that TRT is safe for use in hypogonadal men.
Shores, et al. in 2012 conducted a retrospective cohort study to investigate the link between TRT and mortality in men with testosterone deficiency [32]. The study aimed to compare mortality rates in testosterone-deficient men receiving TRT versus those who did not. Of the 1031 men with low testosterone levels, 398 men (39%) received TRT. The mortality rate in the untreated group was approximately twice that of the treated group (3.4 vs. 5.7) deaths per 100 person-years. Thus, TRT use in testosterone-deficient men was associated with decreased mortality (hazard ratio 0.61, confidence interval 0.42-0.88, P = 0.008). Age, coronary artery disease, and DM did not affect the outcome significantly.
A retrospective study led by Sharma with a team of researchers studied 83,010 veteran hypogonadal men investigating the link between CV events and all-cause mortality (in participants with no history of stroke or MI) and normalization of total testosterone after TRT use [33]. Eligible participants were grouped into normalized-TRT (43,931 men), non-normalized-TRT (25,701 men), and non-TRT (13,378 men). Comparing the groups, normalized-TRT had a lower risk of stroke (HR: 0.64, CI 0.43-0.96), MI (HR: 0.76, CI 0.63-0.93), and all-cause mortality (HR: 0.44, CI 0.42-0.46) compared to non-TRT. Normalized TRT also had a lower risk of stroke (HR: 0.70, CI 0.51-0.96), MI (HR: 0.82, CI 0.71-0.95), and all-cause mortality (HR: 0.53, CI 0.50-0.55) compared to non-normalized-TRT. It was concluded that long-term use of TRT may decrease the risk of stroke, MI, and all-cause mortality in hypogonadal men with normalized serum testosterone and no history of stroke or MI.
Another retrospective cohort study was published in 2016, which was to evaluate the effects of long-term TRT use on CV outcomes, specifically MACE (composite of death, nonfatal stroke, and nonfatal MI) [34]. It was observed that out of the 4,736 men treated, 2,241 men were found to have normal testosterone levels between 212-742 ng/dl and this set of men had better 3-year MACE outcomes primarily for all-cause death compared to 801 men with persistently low testosterone less than 212 ng/dl. The three-year MACE HR was non-inferior but not superior for those with high testosterone (> 742 ng/dl, n = 1,694) compared to those with persistently low testosterone (HR: 0.77, CI 0.54-1.04, P = 0.09). Those with high testosterone did not achieve non-inferiority for MACE compared to those with normal testosterone (HR: 1.20, CI 0.82-1.78). The study found a trend for higher stroke rates in those with high serum testosterone compared to those with persistently low serum testosterone, although there was no CV benefit on MI rate. The study also found that those aged < 65 years with persistently low serum testosterone had higher MACE and mortality.
An observational study investigating long-term TRT effects among 77 hypogonadal men with a history of CVD who received IM testosterone undecanoate every 12 weeks for eight years found that TR significantly decreased weight, BMI, and WC whilst improving their cardio metabolic profiles [35]. Interestingly, there were no MACEs suffered by any participants throughout the study period. Long-term TRT appears to be effective in improving cardiometabolic risk factors in hypogonadal men with a history of CVD and may be an effective add-on medication for secondary prevention of CV events.
However, the story changes in a retrospective study done by Vigen, et al., [36] which was to examine the relationship between TRT and MI, stroke and all-cause mortality among 8709 male veterans with low serum testosterone who underwent coronary angiography and to determine if CV events are modified by underlying coronary artery disease (CAD). In this study, only 1223 patients received TRT. The study followed up the cohort for 531 days and found a higher incidence of adverse outcomes in patients who received TRT (HR: 1.29, CI 1.04-1.58). The Kaplan-Meier estimated cumulative percentage events were 25.7% in the testosterone group and 19.9% in the non-testosterone group with an absolute risk difference of 5.8% (CI -1.4% to 13.1%) after three years of coronary angiography. Study participants had serious CV risks, including coronary artery disease with 20% or more stenosis, obesity, hyperlipidaemia, hypertension, congestive heart failure, COPD, obstructive sleep apnoea, and peripheral arterial disease. This could account for the increased CV events and mortality documented.
Aversa and colleagues studied the effects of testosterone replacement therapy (TRT) in 50 men with low testosterone and metabolic syndrome [37]. Participants were randomized to receive either 1000 mg of parenteral testosterone undecanoate every 12 weeks or a3-6g placebo gel per day for 24 months. TRT led to significant improvements in waist circumference, visceral fat mass, HOMA-IR, CIMT, and hs-CRP compared to the placebo group. A similar study [38] showed that long-term TRT with IM testosterone undecanoate every three months for 36 months led to a 5% increase in bone mass per year with reductions in hs-CRP (2.6 ± 1.8 at baseline to 2.1 ± 1.2 at 36 months, p = 0.001) and WC (109 ± 3 at baseline to 96 ± 5 at 36 months, p < 0.0001) over 36 months. This study showed the benefit and safety of long-term use of TRT although the sample size is small.
A clinical trial by Basaria, et al., [2] which studied testosterone’s effects on Atherosclerosis Progression in Ageing Men (TEAAM) examined the long-term effects of TRT on subclinical atherosclerosis progression in older men with low testosterone levels with the primary outcome measures being carotid intima-media thickness (CIMT) and coronary artery calcium. Out of 1893 identified participants, only 308 were randomized into the study (1:1) to the intervention medication (7.5g of 1% testosterone gel) or placebo gel daily for three years. The rate of change in the CIMT was 0.012 mm/year in the intervention group and 0.010 mm/year in the placebo group (mean difference adjusted for age and trial size, 0.0002 mm; 95% CI -0.003 to 0.003, p = 0.89). The rate of change in the coronary artery calcium score was 31.4 Agatston unit/year in the intervention group, while it was 41.4 Agatston unit/year in the placebo group (mean adjusted difference is -10.8 Agatston unit/year; 95%CI -45.7 to 24.2, p = 0.54). Adverse effects did not differ between the two groups except for increased erythrocytosis and PSA in the intervention group. The study did not find significant differences in CIMT or coronary artery calcium scores between the TRT and placebo groups over three years being that a 0.03 mm increase in CIMT led to a relative risk ratio of coronary death or nonfatal MI of 2.2 with a risk of coronary artery disease events being 3.3.
Strengths of the reviewed studies include long-term use of TRT in men with hypogonadism across multiple sites and continents, with RCTs and cohort studies highlighting the beneficial effects of TRT on CV risk factors (e.g., reduced WC, weight, HbA1c, and improved lipid parameters) and CVD outcomes such as previous MI, coronary disease, obesity, T2DM, and all-cause mortality in men with LOH and FH.
Some limitations identified in the review were:
• Ethical issues in some studies resulted in mixed study designs and lack of blinding, leading to performance bias [18,25,26].
• Selection bias was present in some studies due to unmatched study groups and specific study populations. As noted in some of the studies [30,36] some of the deducted reasons were probably due to unmatched study groups and the use of a very specific study population (people who have had angiography procedures).
• Supply interruption of testosterone and inability to source other medications affected some studies [28,30,35].
• Lack of standardization in dosing of the testosterone therapy used [19] and methods of assessing adherence to diet and medication [27]. There was also the absence of data on the rationale for the choice of TRT and the type of formulation.
• Majority of the trials and observational studies did not primarily set out to determine the outcome of MACE and mortality. In the few studies where CV events were the primary outcome, there were inconsistencies in the severity assessment of CV events.
• Small sample sizes of RCTs may limit the generalization of results to larger populations [22,38].
• High drop-out rate or Lost-to-follow-up rate were observed in some studies such as TEAAM [2], Times 2 trial [22]. Some of the reasons for the high rate of dropout or loss of follow-up ranged from adverse drug reactions to personal reasons. One of the studies which used intramuscular testosterone in the clinical trial [38] had a dropout rate as high as 50%.
• Absence of placebo-treated or control group limits interpretation and generalization of results [29,35,38].
• One of the retrospective studies [36] had potential unmeasured confounding biases, despite the use of a statistical (non-parsimonious) model to minimize residual confounders. This may result in errors in testosterone errors.
Evidence from RCTs and observational studies suggests that untreated LOH and FH in men increase the risk of CV events and all-cause mortality. Low testosterone may signal vascular dysfunction associated with cardiovascular disease and erectile dysfunction, especially when coupled with cardio metabolic risk factors. Long-term TRT can decrease CV risk factors, post-CV events, and all-cause mortality in hypogonadal men, particularly when restoring serum testosterone levels to normal limits. However, men with LOH and FH who have higher serum testosterone levels due to TRT may be at a higher risk of stroke events [28,34].
Testosterone replacement therapy can improve weight, WC, hepatic steatosis, blood pressure, lipid parameters, HOMA-IR, HbA1c, ED, BMD, insulin resistance, glycaemic control, and endothelial function, and reduce surrogate markers of endothelial dysfunction and atherosclerosis progression [17,37,38]. Long-term topical TRT does not worsen CV risk factors or events, while IM testosterone undecanoate provides tremendous CV benefits when used safely. Additionally, improvements in cardiometabolic and hormone profiles may be lost after TRT withdrawal [27]. Observational studies investigating the effects of long-term topical use of TRT have not shown any worsening of cardiovascular risk factors or events, and no increase in all-cause mortality in men with hypogonadism. In contrast, studies that had IM testosterone undecanoate showed tremendous CV benefits especially when safe practices are followed. Thus, Long-term TRT use may be an effective secondary prevention medication for hypogonadal men with a history of CVD. Still, caution is advised for elderly hypogonadal men with established CVD.
Larger RCTs and observational studies are still needed, focusing on MACE and all-cause mortality outcomes in men with LOH and FH, especially among those with anabolic steroid-induced hypogonadism and excessive exercise-induced hypogonadism on long-term TRT.
Cardiovascular safety, MACE, and all-cause mortality have received little attention in studies on the long-term use of TRT in men with LOH and functional hypogonadism. The systematic review identified various study designs, eligibility criteria, and outcomes, resulting in wide heterogeneity in methods. Applying study findings to the general population will be challenging. Table 3 provides a protocol for uniform monitoring of the efficacy and safety of TRT in studies involving LOH and FH [39].
Table 3: Checklists for monitoring the efficacy and safety of TRT in men with LOH and functional hypogonadism. View Table 3
The research aims to determine cardiovascular risks, benefits, and events (especially MACE) associated with TRT use in men with LOH and FH. RCTs and cohort studies are possible study designs to address this question.
Men with symptoms and signs of testosterone deficiency and low serum total or free testosterone concentrations, excluding those with low-normal serum testosterone, should be the case definition for LOH and FH [2]. Total or free testosterone should be measured twice in the morning while fasting, with total testosterone < 320 ng/dl (11 nmol/L) and free testosterone < 64 pg/mL (220 pmol/L) as threshold values.
Figure 2 shows an algorithm for monitoring the safety and efficacy of TRT.
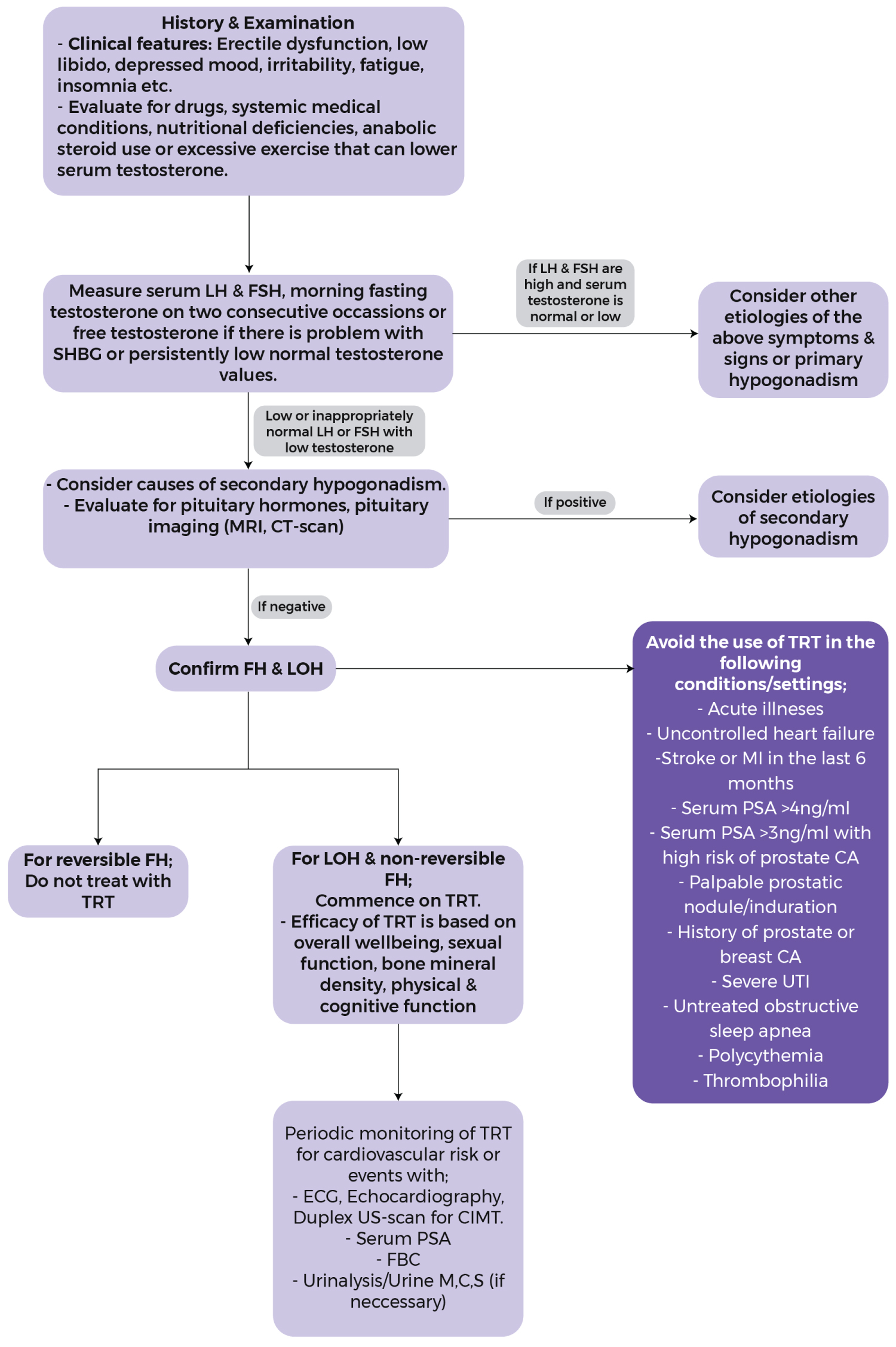 Figure 2: Efficacy & safety of testosterone replacement therapy in late onset hypogonadism & functional hypogonadism.
View Figure 2
Figure 2: Efficacy & safety of testosterone replacement therapy in late onset hypogonadism & functional hypogonadism.
View Figure 2
There is no conflict of interest that could be perceived as prejudicing the impartiality of the research reported.
This research did not receive any specific grant from any funding agency in the public, commercial or not-for-profit sector.
I would like to appreciate and thank Prof Atul Kalhan for his mentorship right from conception to the end of this review. I also want to thank Drs. Ifedayo Odeniyi, Olufemi Fasanmade, Sekinat Adejumobi and Nora Ijeh for their strong support throughout the writing and final approval of the review. I would also like to thank Merck Foundation and University of South Wales for the opportunity to do this work.
Conceived and designed the study: O.B. Olopade and A. Kalhan, Collected the data: O.B. Olopade, S.A. Adejumobi, I.A. Odeniyi, I.N. Ijeh. O.A FasanmadeAnalysing of the results: O.B. Olopade, S.A. Adejumobi, I.A. Odeniyi, I.N. Ijeh, O.A. Fasanmade. A. Kalhan Writing of the manuscript: O.B. Olopade. Revision and approval of the final draft: O.B. Olopade, I.A. Odeniyi, S.A. Adejumobi, I.N. Ijeh, O.A. Fasanmade, A. Kalhan.