Aim: The aim of the present study is to evaluate the alterations and clinical significance of plasma lipid profiles in untreated head and neck malignancies.
Methods: The present case-control study comprises of newly diagnosed and histologically confirmed, 50 head and neck cancer cases between 2021-2022 in the Department of Otorhinolaryngology and Head and Neck Surgery, Tishreen University Hospital, Lattakia, with 25 healthy controls. Fasting blood samples were collected and the lipid profile studied and compared between groups in terms of mean and standard deviation.
Results: The mean difference in the levels of total cholesterol (TC), high-density lipoprotein (HDL), low-density lipoprotein (LDL), very-low-density lipoprotein (VLDL), and triglyceride (TGL) between the case group and control group was significant in our study, that is, these lipid parameters were significantly lower in the case group than that of the control group.
Conclusion: The lower plasma lipid status may be a useful indicator for initial changes occuring in neoplastic cells.
Lipid profile, Head and neck cancers, Squamous cell carcinoma, Grades of tumour differentiation, Smoking
Cancer is one of the leading causes of death worldwide [1]. Head and neck cancers accounts the seventh cancer by incidence [2], which encompass a group of malignancies that arise in the mucosal surfaces of the upper aerodigestive tract (UADT), including the oral cavity, pharynx, larynx, nasal cavity and paranasal sinuses, as well as cancers of the major and minor salivary glands, and recently, skin cancers that start in head and neck region (other than melanoma and Merkel cell carcinoma) was classified as type of head and neck cancer [3,4]. About 90% of all head and neck cancers are squamous cell carcinoma (HNSCC) and strongly associated with certain environmental and lifestyle risk factors such as tobacco and alcohol consumption [5]. One of the hallmarks of cancer is an altered lipid metabolism [6], that is the newly proliferating tumor cells would need many basic components, one such component is lipids [7], which are highly complex molecules that play important roles as a structural component of membrane walls as well as acting as a source of energy and as signaling molecules [8]. Thus, the serum lipid profile is considered one of the various biochemical markers available for precancer and cancerous patients [1]. Usefulness of variations in blood cholesterol levels in diagnosis and treatment of various diseases including cancers has been studied by several researchers [9-12], but only a few reports are available in head and neck malignancy.
The objective of the present study is to evaluate the alterations and clinical significance of plasma lipid profiles in untreated head and neck malignancies and the association with histopathological grade and smoking.
This was a case-control study.
A total number of 75 patients were involved in the study:
Patients with head and neck cancers: 50
Normal controls: 25
The present study was conducted in the Department of Otorhinolaryngology and Head and Neck Surgery, Tishreen University Hospital, Lattakia, Syria.
The study period was from July 2021 to July 2022.
All cases diagnosed clinically as head and neck cancers and confirmed by histopathological examination.
· Obese and those with history of hypertension, diabetes mellitus, coronary artery disease and myocardial infarction.
· Patients having any cardiac, renal and hepatic dysfunction.
· Those on chemotherapy and radiotherapy.
· Those on drugs interfering with lipids.
Healthy subjects with normal hepatic, renal, cardiac function and had no compliant or history of any major illness in recent past.
Routine head and neck examination was carried out on all subjects.
Fasting blood samples were collected and the lipid profile studied for these parameters: TC, HDL, LDL, VLDL, TGL Very low density lipoprotein: calculated by the formula.
» VLDL = Triglyceride / 5 and Low density lipoprotein: by the formula » LDL = Total cholesterol-(VLDL-HDL)
Histopathologically, head and neck malignancy was divided on the basis of their degree of differentiation: Well differentiated, Moderately differentiated , Poorly differentiated, and Undifferentiated.
Statistically: P < 0.05 was considered as the level of significance.
In the present study, among the 50 cases of head and neck malignancy, 35(70%) were males and 15(30%) were females, male to female ratio was 2.33:1.
In the present study, among the 50 cases of head and neck malignancy, the majority of cases 26(52%) were in the age group of 41-60 years, followed by 12(24%) cases in the age group of 21-40 years, 10(20%) cases in group more than 60 years and minimum number of cases 2(4%) was up to 20 years.
It was observed that the larynx (40%) was the most common site of malignancy, followed by oral cavity (24%), pharynx (14%), skin cancers (10%), nasal cavity and paranasal sinuses (8%), and salivary glands (4%) (Figure 1).
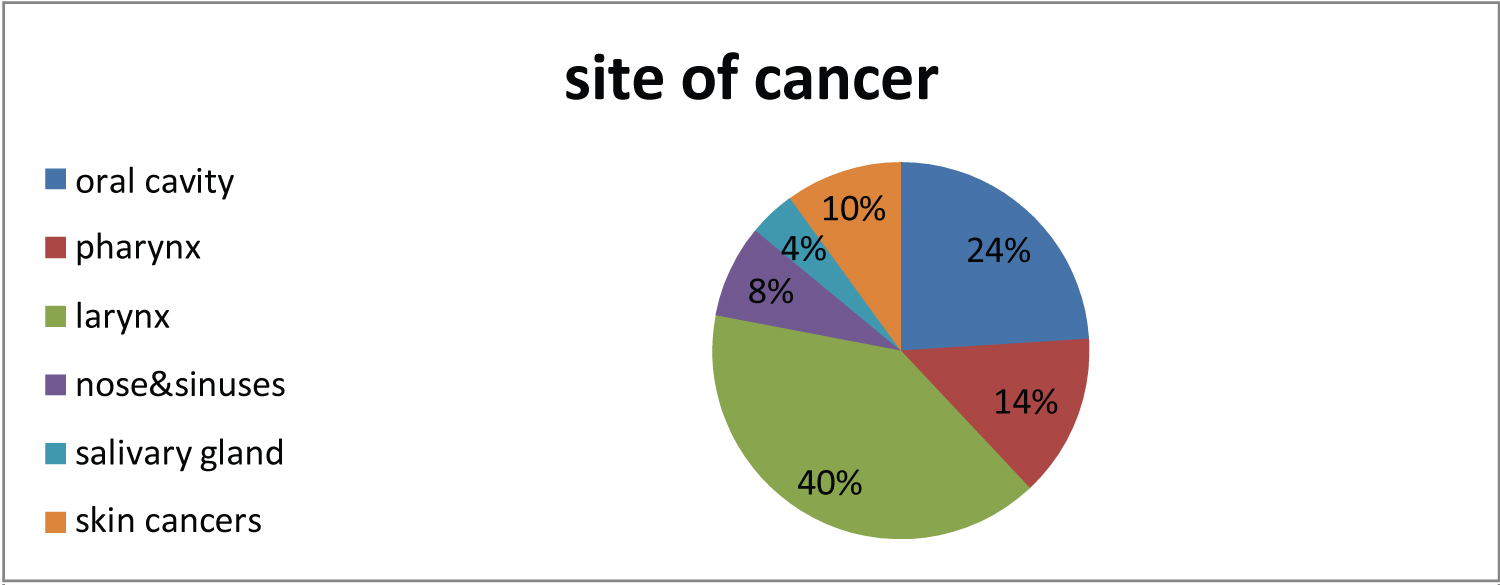 Figure 1: Distribution of study cases according to site of cancer.
View Figure 1
Figure 1: Distribution of study cases according to site of cancer.
View Figure 1
Most of our study cases (44%) were histopathologically graded as moderately differentiated, (28%) well differentiated, (18%) poorly differentiated, and (10%) were undifferentiated (Figure 2). The intergroup evaluation of serum lipid profile levels among various grades of differentiation did not show a significant correlation of serum lipid profile and the degrees of differentiation.
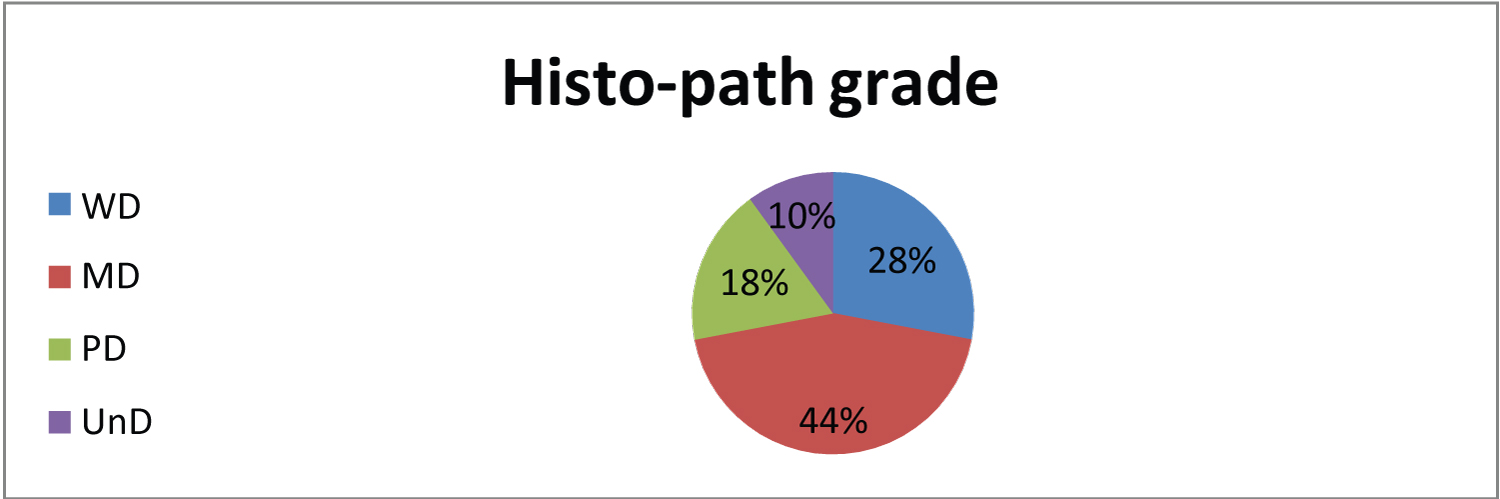 Figure 2: Distribution of study cases according to histopathological grade.
View Figure 2
Figure 2: Distribution of study cases according to histopathological grade.
View Figure 2
The mean serum lipid profile values of cases with head and neck malignancy and control groups are represented in (Table 1). The P values are < 0.01 for all parameters , suggesting that, statistically, there is a highly significant reduction of mean serum TC, HDL, LDL, VLDL, and TGL in the subjects of head and neck malignancy as compared to control group. We observed that maximum of cancer patients 45(90%) were smokers, and only 5(10%) had no habit of smoking. The plasma lipid levels were compared between cancer patients with habit of smoking and without habit of smoking and the results did not show a significant difference between the two groups (P > 0.05), but when plasma lipid levels were compared between cancer patients with habit of smoking and controls with habit of smoking, TC, HDL, LDL, VLDL, and TGL were found significantly lower in subjects with head and neck malignancy with habit of smoking (P < 0.05) (Table 2).
Table 1: Lipid profile in head and neck cancers versus controls. View Table 1
Table 2: Comparison of lipid profile with habit of smoking. View Table 2
The new tumor cells would need many basic components for their proliferation, one of these components is lipids which form major cell membrane components, essential for various biological functions [ ، 13], not only for providing the membrane constituents of proliferating cells , but are also needed for energetic, biophysical, and signaling pathways that drive tumorigenesis. Dysregulated lipid metabolism is a hallmark of cancer [14], as the variations in blood cholesterol levels have been studied by several researchers who have reported association of plasma lipids and lipoproteins with different cancers [15,16] including head and neck cancers, but the question of whether hypolipidemia at the time of diagnosis is a causative factor or a result of cancer is still controversial. There are three competing hypotheses to explain this inverse association. First, lower cholesterol values, even before the manifestation or detection of cancer, may be a result of the cancer process; second, lower cholesterol values may precede the development of cancer, but the association with cancer is secondary, which indicates that cholesterol serves as a marker for some other causal variable or set of variables; third, lower cholesterol values may precede the development of cancer and may be causally associated with the occurrence of some forms of cancer [17].
The mean serum lipid profile values in our present study showed P values < 0.01 for all parameters, suggesting statistically, a significant reduction of mean serum TC, HDL, LDL, VLDL, and TGL in the head and neck malignancy cases as compared to control group. This is in accordance with the study conducted by Agrawal, et al. [1], while Sabea [18] and Poorey and Thakur [19] found a significant reduction only in TC and HDL levels. Vyas, et al. [20] found a significant reduction in all lipid parameters except HDL. Meena, et al. [5] found a significant reduction in all lipid parameters except VLDL. The results of our study were in accordance with the studies conducted by Meena, et al.; Poorey and Thakur and Wilms, et al . [5,19,21] who found no statistically significant correlation of lipid profile with the grade of tumor differentiation.
In the present study, when the mean serum TC, HDL, LDL, VLDL and TGL levels between head and neck cancer group with no habit of smoking and with habit of smoking were compared, there was no statistically significant difference in their levels, but when the serum lipid levels of cancer patients with habit of smoking were compared with the serum lipid profile levels of controls with habit of smoking to eliminate any bias because of smoking habit, significant lower levels of mean TC, HDL, LDL, VLDL and TGL were found in cancer patients group. These findings imply that lower lipid levels may be mainly because of the basic underlying disease process and not because of smoking habit. This suggests that although the role of tobacco has been established as an etiological factor for head and neck cancer, it may not have a direct and overall significant association with serum lipid levels [22]. This result was in accordance with a study conducted by Wilms, et al. [21], while Meena, et al . [5] found a significant reduction in TC and LDL levels in patients with habit of smoking.
The results of the present study showed an evidence of an inverse relationship between the serum lipid profile and head and neck malignancy, and this supports the fact that lipid profile levels can be used as a diagnostic parameter for early detecting of cancer.
We wish to thank all medical staff in Otorhinolaryngology Department at Tishreen University Hospital for their hard work even with great difficulties.
None.
The authors declare that they have no conflict of interests.