Plasma cell neoplasms are derived from terminally differentiated B-cells. The distinction between anaplastic plasma cell myeloma and plasmablastic lymphoma, a B cell lymphoma, can be challenging. We present 3 cases of neoplasms with plasmacytic features that highlight the heterogeneity of plasma cell neoplasms and challenges in their diagnosis. Molecular profiling of these cases may provide value in their differential diagnosis.
A 60-year-old male with a persistent headache was transferred to the neurology clinical team. CT head demonstrated an avidly enhancing intracranial lesion of the frontal lobe, measuring 6.1 × 4.8 cm, with no herniation or midline shift. No lesions were seen in the chest, abdomen or bones on further imaging. Laboratory data showed a normal CBC and electrolytes and negative serology. No paraprotein was noted on serum protein electrophoresis. Past medical history was significant for hypertension and hidradenitis suppurativa. There was no history of immunosuppression. A craniotomy and biopsy of the lesion was performed. Histologic sections demonstrated a diffuse sheet of large lymphoid cells with immunoblastic features, brisk mitoses, and apoptotic bodies. There were focal areas of tumor necrosis. Immunohistochemistry showed positive staining for CD45, MUM1 and CD138, with lack of expression of pan-B cell markers (CD20, CD79a, PAX5), and T cell markers (including CD3 and CD5). There was no expression of CD34, CD56, CD10, BCL6 and CD30. HHV-8 and EBER-ISH were negative. Molecular studies for myc, bcl2 and bcl6 gene rearrangements showed myc gene rearrangement. The case was diagnosed as plasmablastic lymphoma. PET-CT scan for staging was negative. Bone marrow biopsy indicated a morphologically and immunophenotypically normal marrow, with no evidence of involvement by lymphoma. Bone scans were negative, thus excluding the considered differential diagnosis of anaplastic plasma cell myeloma. The clinical team chose to initiate steroid and palliative care measures. Figure 1: H&E showed diffuse sheets of large lymphoma cells with immunoblastic features and brisk mitoses (Figure 1A). These were positive for CD138 (Figure 1B) with high ki67 proliferative index of 95% (Figure 1C) and negative EBER-ISH (Figure 1D).
 Figure 1: H&E showed diffuse sheets of large lymphoma cells with immunoblastic features and brisk mitoses (Figure 1A). These were positive for CD138 (Figure 1B) with high ki67 proliferative index of 95% (Figure 1C) and negative EBER-ISH (Figure 1D).
View Figure 1
Figure 1: H&E showed diffuse sheets of large lymphoma cells with immunoblastic features and brisk mitoses (Figure 1A). These were positive for CD138 (Figure 1B) with high ki67 proliferative index of 95% (Figure 1C) and negative EBER-ISH (Figure 1D).
View Figure 1
A 67-year-old female presented with a 6 month history of worsening pressure-like pain in the right eye, headache, and exophthalmos, initially attributed to a refractory headache. Physical examination revealed decreased visual acuity in the right eye and a third cranial nerve palsy. Social history was significant for daily alcohol consumption and former smoking history with an unspecified number of pack years. She had an ECOG performance status of 0 (fully active, able to carry on all pre-disease performance without restriction) and no significant past medical history. CT and MRI revealed a right cavernous sinus mass, with intraosseous extension into the right sphenoid bone, and compression of the right optic nerve. CT chest, abdomen, and pelvis showed no evidence of adenopathy or lymphoma. CBC and electrolytes were within normal reference range. Serum protein electrophoresis did not demonstrate any serum paraprotein.
The sphenoid mass was biopsied with microscopy revealing diffuse infiltrates by atypical lymphoid cells with plasmacytoid features. The nuclei demonstrated moderate pleomorphism. Mitotic and apoptotic activities were not increased. There were no foci of necrosis. There were background infiltrates of small lymphocytes. By immunohistochemistry, lesional cells were positive for CD45, CD138, MUM1, CD79a, and EMA (weak). They were negative for PAX5, CD20, CD3, CD5, CD30, myc, pan keratin and GFAP. Kappa and lambda stains demonstrated kappa light chain restriction. The Ki67 proliferation index was 20%. Molecular studies for myc, bcl2 and bcl6 gene rearrangements were negative. Subsequent bone marrow biopsy was negative for involvement by myeloid, lymphoid or plasma cell neoplasm. A diagnosis of EBV positive plasmacytoma in an immunocompetent patient (EPIC) was made.
Figure 2 shows diffuse sheets of plasmacytoid cells (Figure 2A) that stain positive for CD138 (Figure 2B) with a Ki-67 proliferative index of 20% (Figure 2C). EBER-ISH is positive (Figure 2D), and they are kappa light chain restricted (Figure 2E), with minimal lambda light chain expressivity by ISH (Figure 2F).
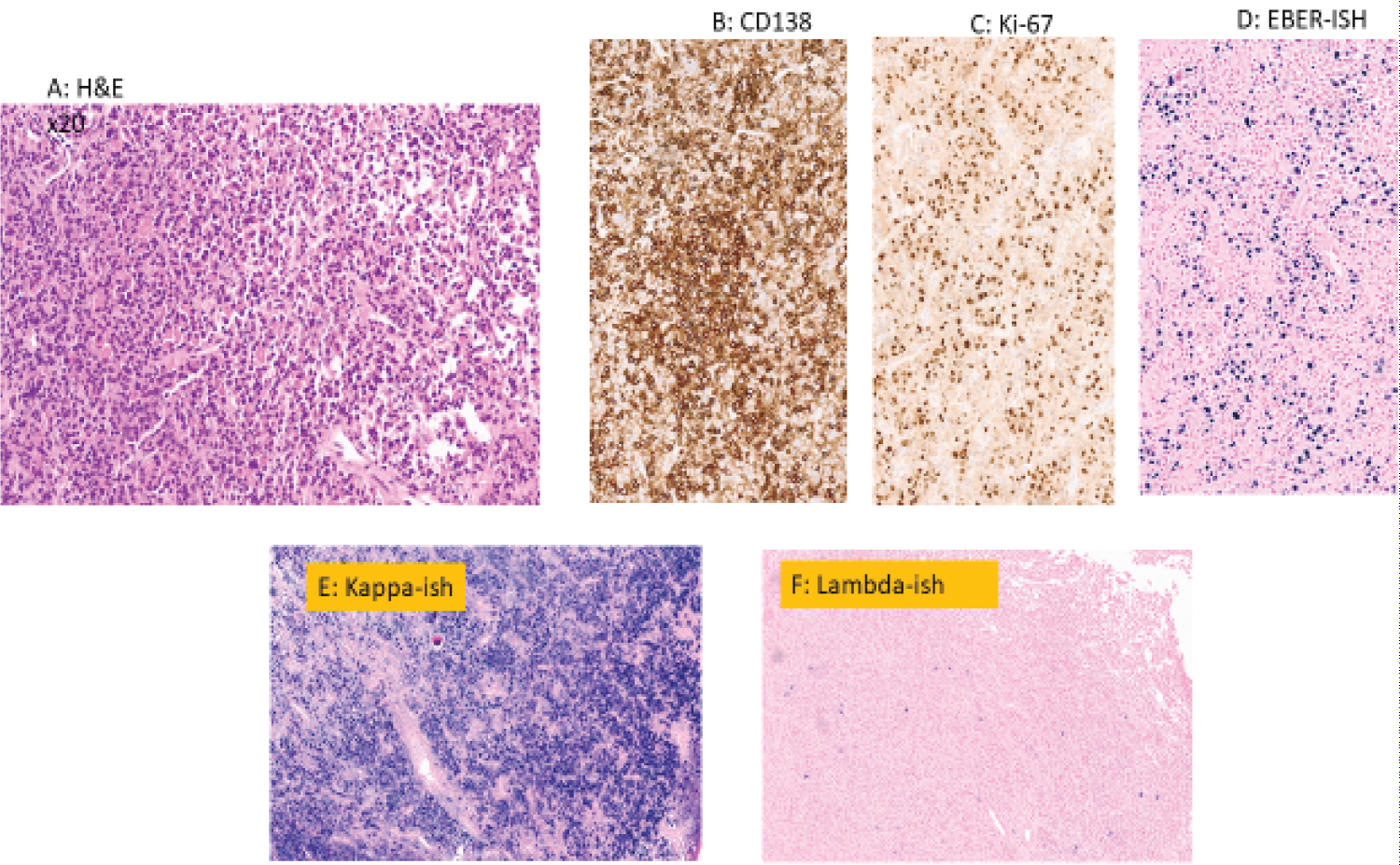 Figure 2: Shows diffuse sheets of plasmacytoid cells. (Figure 2A) that stain positive for CD138 (Figure 2B) with a Ki-67 proliferative index of 20% (Figure 2C). EBER-ISH is positive (Figure 2D), and they are kappa light chain restricted (Figure 2E), with minimal lambda light chain expressivity by ISH (Figure 2F).
View Figure 2
Figure 2: Shows diffuse sheets of plasmacytoid cells. (Figure 2A) that stain positive for CD138 (Figure 2B) with a Ki-67 proliferative index of 20% (Figure 2C). EBER-ISH is positive (Figure 2D), and they are kappa light chain restricted (Figure 2E), with minimal lambda light chain expressivity by ISH (Figure 2F).
View Figure 2
A 70-year-old male with IgA serum paraprotein presented with a pain crisis. He was found to have normocytic anemia, mild renal insufficiency, and mild hypercalcemia. Additionally, there was elevated beta-2 microglobulin, hypoalbuminemia, and elevated LDH. Bone marrow biopsy showed extensive clonal (kappa light chain restricted) neoplastic plasma cells. FISH performed on the bone marrow aspirate revealed multiple genetic abnormalities, including loss 1p, gain 1q, +11, gain IGH, -16, and -TP53. CT showed a left chest wall mass measuring up to 3.0 cm in maximal dimension. This was biopsied and microscopy showed diffuse sheets of poorly differentiated lymphoid cells with plasmablastic features and increased mitoses. By immunohistochemistry, lesional cells were positive for CD138 (weak to moderate staining), MUM1, CD30 (strong and diffuse), BCL2 and high ki-67 proliferative index (over 95%). Neoplastic cells were negative for CD20, CD79a, PAX5, CD3, CD5, ALK1, CD56, BCL6, CD10 and EBER-ISH (Figure 3). The patient was treated with a regimen including Isatuximab, Carfilzomib and Dexamethasone.
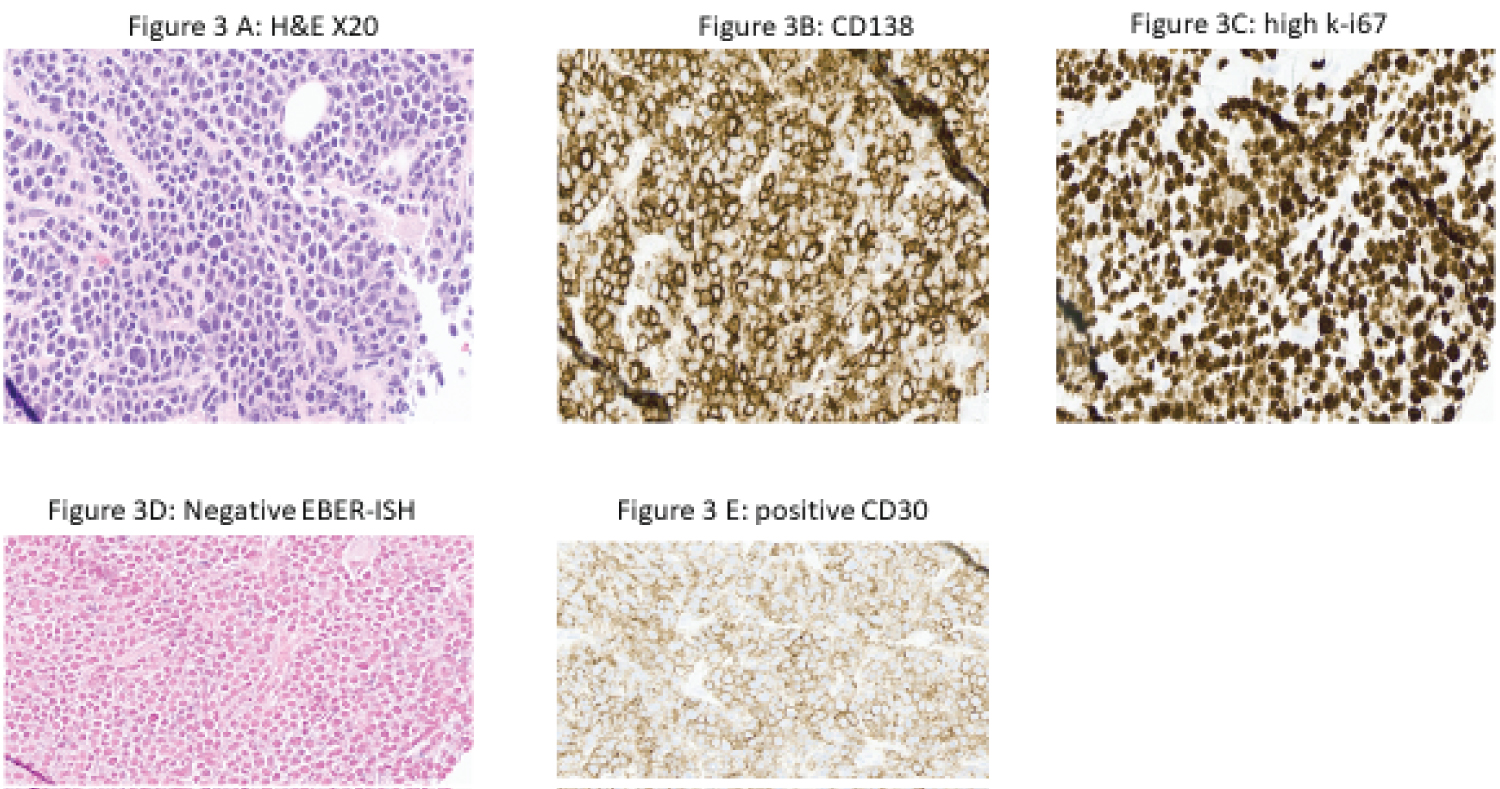 Figure 3: Shows diffuse infiltrates of poorly differentiated cells on H&E, positive for CD138 (Figure 3B) and high ki67 proliferative index of 90% (Figure 3C). EBER-ISH was negative (Figure 3D) and CD30 was expressed (Figure 3E).
View Figure 3
Figure 3: Shows diffuse infiltrates of poorly differentiated cells on H&E, positive for CD138 (Figure 3B) and high ki67 proliferative index of 90% (Figure 3C). EBER-ISH was negative (Figure 3D) and CD30 was expressed (Figure 3E).
View Figure 3
Figure 3 shows diffuse infiltrates of poorly differentiated cells on H&E, positive for CD138 (Figure 3B) and high ki67 proliferative index of 90% (Figure 3C). EBER-ISH was negative (Figure 3D) and CD30 was expressed (Figure 3E).
Plasma cell neoplasms are derived from terminally differentiated B-cells. These include multiple myeloma, localized plasma cell tumors that lack significant bone marrow infiltration (including solitary plasmacytoma of bone and primary extra-osseous/extramedullary plasmacytoma) and disorders primarily characterized by the consequences of abnormal immunoglobulin deposition, namely immunoglobulin light chain amyloidosis and non-amyloid light and/or heavy chain immunoglobulin deposition diseases [1,2]. The distinction between anaplastic plasma cell myeloma and plasmablastic lymphoma, a B cell lymphoma, may be challenging. In view of differences in the biological behavior, etiology, treatment and prognosis, it becomes essential to differentiate between these entities.
We present 3 cases of neoplasms with plasmacytic features that highlight the heterogeneity of plasma cell neoplasms and challenges in their diagnosis.
Patient #1 was immunocompetent, with no history of HIV or underlying medical conditions associated with immunosuppression [3,4]. The aggressive microscopic appearance of large lymphoid cells with brisk mitoses and foci of necrosis is compatible with expected phenotype of plasmablastic lymphoma. However, the lack of EBER-ISH expression and immunocompetent status are an unexpected finding. Molecular studies demonstrated myc rearrangement which further supported our diagnosis as plasmablastic lymphoma, EBV negative, in an immunocompetent patient.
Patient #2 met multiple criteria suggesting EBV-positive plasmacytoma of an immunocompetent patient, including low Ki67 index, light chain restriction, no necrosis, and immunocompetent status [5,6]. These often have an indolent clinical course after surgery with radiation or chemotherapy. In view of the few cases reported in literature, it is unclear if this rare tumor may potentially progress to a plasmablastic lymphoma.
Patient #3 is a classic case of an anaplastic variant of multiple myeloma involving the chest wall with a high Ki67 proliferative index and CD30 expression. The extensive marrow involvement and serum paraprotein were also consistent with a diagnosis of multiple myeloma [7,8].
A comparative genomic hybridization study, or molecular profiling of the three tumors described, may further show similarities and differences. Our cases highlight the heterogeneity and unexpected features of cases of plasma cell neoplasms.