Inverted papilloma (IP) may be associated with synchronously or metachronously rhinosinusal squamous cell carcinoma.
To determine the incidence of squamous cell carcinoma in patients with IP of the paranasal sinuses andlocal control in patients treated for cancer associated with IP.
A descriptive and retrospective study was carried out.
All patients who were treated in the rhinosinusology section of the otorhinolaryngology department of the Hospital Italiano de Buenos Aires with histopathology diagnosis of inverted papilloma between January 2005 and December 2021 were included.
Those with associated malignant tumors were selected.
Sixty three patients with a histopathological diagnosis of inverted papiloma were treated.
Five had a synchronous malignant tumors, 4 epidermoid carcinomas and one a verrucous carcinoma and two a metachronous cancer (11.11%).
The treatment included surgery, radiotherapy and chemotherapy combined in different schemes according to the indication of the tumor committee.
The incidence of malignant tumors associated with inverted papilloma found in our study was 11.11% (7 of 63 patients).
Two patients had metachronous and 5 synchronous malignant tumors.
In three patients local control of the disease was obtained.
The prognosis of epidermoid and verrucous carcinoma associated with inverted papilloma is similar to rhinosinusal squamous carcinomas not associated with inverted papilloma.
Inverted papiloma, Epidermoid carcinoma, Methacronic carcinoma, Synchronous carcinoma
Inverted Papilloma (IP) is a benign tumor, locally aggressive, with a tendency to recur after surgery and to present characteristics of malignancy such as dysplasia, carcinoma in situ and invasive carcinoma.
The incidence of the association with carcinoma differs according to different studies (0-53%) [1,2].
In a review of 65 published case series (3181 patients) they reported 10.4% synchronous and metachronous malignancies with inverted papilloma. Most were squamous cell carcinomas [2].
The association of squamous cell carcinoma (EC) with inverted papilloma can lead to confusion and delays in indicating the appropriate treatment.
In this association, the concept of malignancy should prevail and treatment should be similar to that of primary squamous cell carcinoma.
To determine the incidence of squamous cell carcinoma in patients with inverted papilloma of the paranasal sinuses and local control in patients treated for cancer associated with inverted papilloma.
Descriptive and retrospective.
Patients who were evaluated and treated in the Rhinosinusology sector of the Otorhinolaryngology Department of the Italian Hospital of Buenos Aires with histopathological diagnosis of inverted papilloma between January 2005 and December 2021 were included.
Patients with a histological diagnosis of IP associated with squamous cell carcinoma were selected.
The cancer was considered to be synchronous with the IP when it was diagnosed at the same time, and the patient had no history of previous surgery, and metachronous when it occurred after recurrences of the inverted papilloma somewhere where the tumor was.
All the patients were studied by Computed Tomography (CT) of the brain, paranasal sinuses, neck, chest, and abdomen, and/or Positron Emission Tomography (PET) and contrast-enhanced Magnetic Resonance Imaging of the paranasal sinuses (MRI).
Diagnosed squamous cell carcinomas were staged according to the AJCC TNM classification, 8th edition of the year 2018.
The therapeutic decision arose from the recommendations of the hospital tumor committee.
The surgeries were performed by endonasal approach with 0° and 30° endoscopes and in one patient an anterior maxillary sinusotomy was associated.
The radiotherapy technique used was intensity modulated radiotherapy with a total dose of 70gy.
Post-treatment controls were performed by nasal endoscopy, CT, MRI and PET.
Sixty-three patients were treated for inverted paranasal sinus papillomas.
Forty were men and twenty-three women, the youngest was 24-years-old and the oldest 79, the averageage was 49.8 years.
Six of the 63 patients treated for inverted papilomas had epidermoid carcinomas and one a verrucous carcinoma (11.11%).
Five had synchronous and two had metachronous carcinomas.
All consulted for unilateral or bilateral nasal obstruction, one also due to bilateral decreased visual acuity and the other due to unilateral exophthalmos.
The diagnosis of squamous cell carcinoma associated with inverted papiloma was made by the histopathological study of the biopsy performed through endonasal approach and in one by puncture of the frontal sinus.
Synchronous and metachronous carcinomas associated with IP were staged: T4B (2/7), T4A (2/7), T3 (2/7), and T2 (1/7). None presented cervical adenopathies or distant metastases (N0, M0).
Three were treated with concurrent chemotherapy/radiotherapy, two because they were considered inoperable due to the extension of the tumor (T4B) and another because the frontal sinus, meninges and eye ball were involved (T4A) and an attempt was made to preserve the eye.
In one of the T4B patients, local control of the Disease was achieved during a 5-year follow-up, and another died 6 months later with residual local disease.
The patient with EC T4A with involvement of the eye had a cognitive deterioration after finishing the treatment with chemoradiation therapy, for which he was not rescued with surgery and was left with residual disease and palliative treatment.
In three of the four patients treated with surgery, postoperative radio therapy was indicated (T4A and T3: 2/3).
One of them died after surgery during treatment with chemo-radiotherapy (T4A).
There maining three live without locoregional or distant disease, with a 5-year follow-up in two and a 1-year follow-up in another.
Local control at 5 years was obtained in 3 patients (42.85%) (Table 1, Figure 1, Figure 2, Figure 3, Figure 4, Figure 5, Figure 6 and Figure 7).
 Figure 1: Synchronous squamous cell carcinoma with inverted papilloma T4-B.
Figure 1: Synchronous squamous cell carcinoma with inverted papilloma T4-B.
MRI - A, B, C: A tumor is observed that invades the endocranium, compromising the optic chiasm and extending to the lateral wall of then as opharynx, D: MRI where the disappearance of the tumor is observed after treatment with CT/RT.
View Figure 1
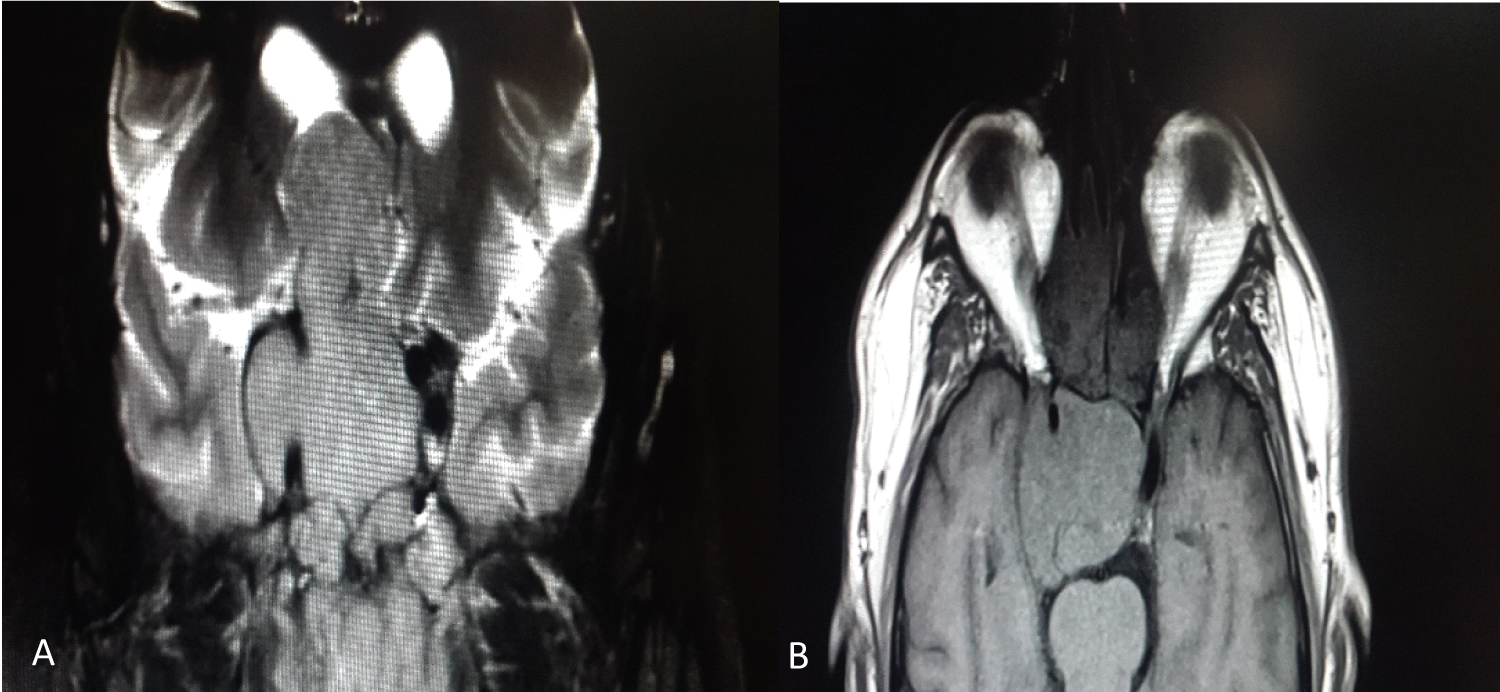 Figure 2: Synchronous squamous cell carcinoma with inverted papilloma T4B (A, B) MRI showing an extensive tumor with intracranial invasion. He under went treatment with CT + RT and died of local disease.
View Figure 2
Figure 2: Synchronous squamous cell carcinoma with inverted papilloma T4B (A, B) MRI showing an extensive tumor with intracranial invasion. He under went treatment with CT + RT and died of local disease.
View Figure 2
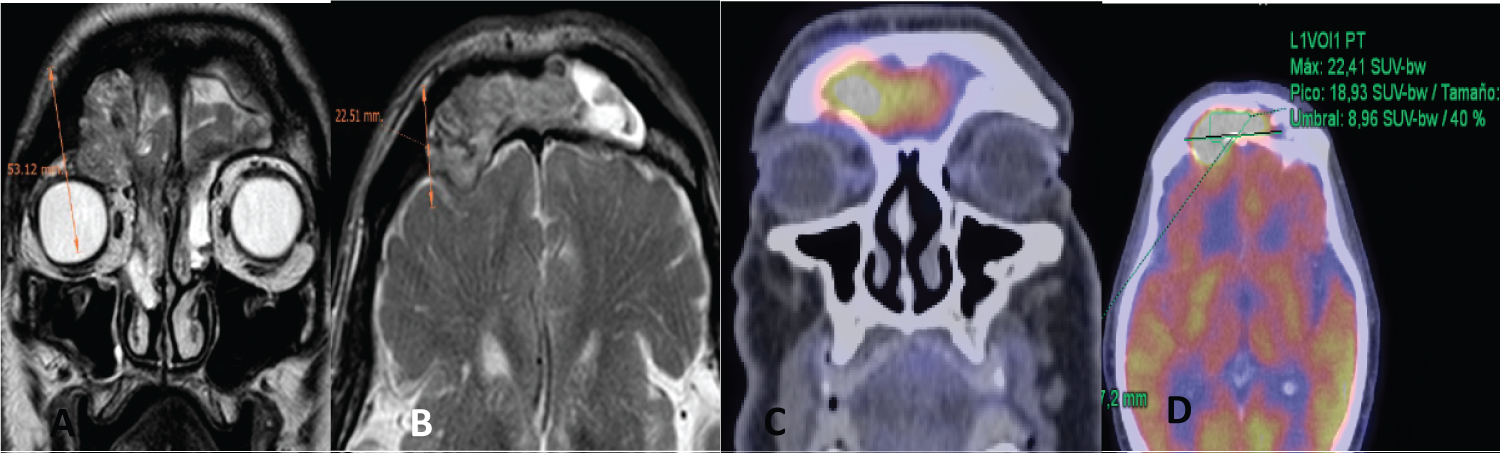 Figure 3: Metachronous squamous cell carcinoma with IP of frontal sinus.
Figure 3: Metachronous squamous cell carcinoma with IP of frontal sinus.
(A) Coronal MRI: involvement of the lateral and superior periorbita is observed; (B) Axial MRI: Extradural endocranial invasion with posible involvement of the meninges; (C and D) PET with frontal uptake. He did CT+ RT, and could not be rescued with surgery due to cognitive impairment.
View Figure 3
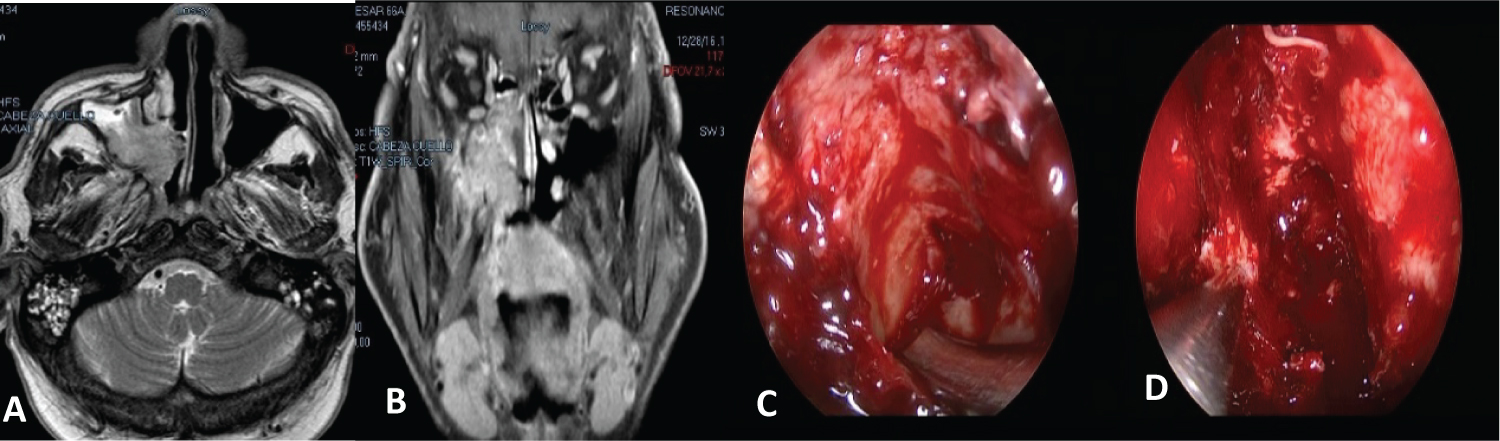 Figure 4: (A and B) MRI: A tumor is observed that compromisos the posterior wall of the maxillary sinus with extension to the pterygom axillary fossa and bone invasion of the ethmoid roof; (C, D) Endonasal view with endoscopes at the end of surgery. He did postoperative CT + RT.
View Figure 4
Figure 4: (A and B) MRI: A tumor is observed that compromisos the posterior wall of the maxillary sinus with extension to the pterygom axillary fossa and bone invasion of the ethmoid roof; (C, D) Endonasal view with endoscopes at the end of surgery. He did postoperative CT + RT.
View Figure 4
 Figure 5: Synchronous squamous cell carcinoma with IP (T3N0M0).
Figure 5: Synchronous squamous cell carcinoma with IP (T3N0M0).
(A) MRI: Tumor occupying the nasal cavity, ethmoid and maxillary sinus with erosion of the posterior wall; (B) Endoscopic view of the tumor in the nasal cavity; (C) Tumor in the posterior wall of the maxillary sinus; (D) Drilling of the bone and resection of the posterior wall of the maxilla; (E) Postoperative CT.
View Figure 5
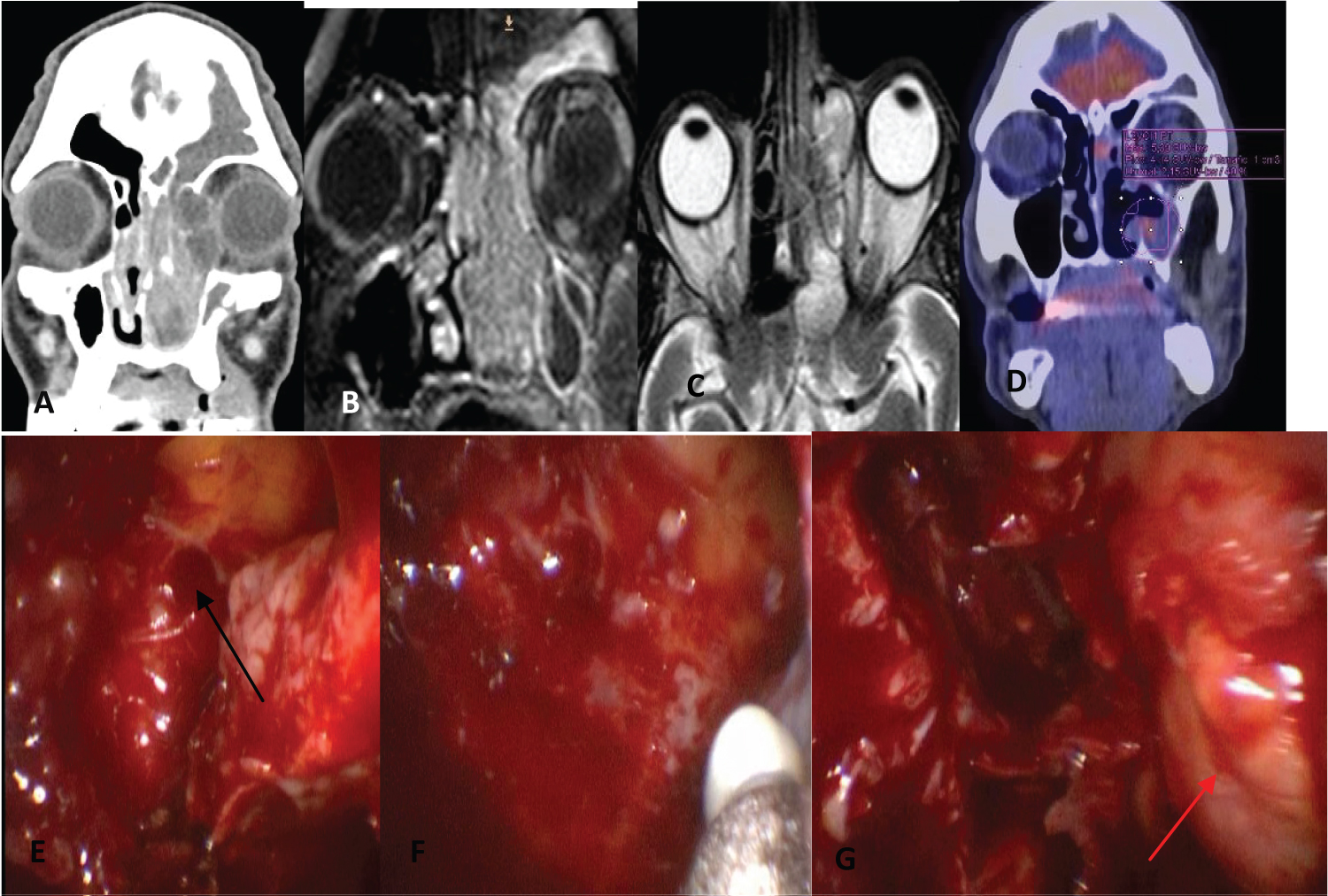 Figure 6: Synchronous squamous cell carcinoma with IP (T3N0M0). (A) CT showing the tumor in the nasal cavity and the involvement of the innerwall of the orbit; (B) Coronal MRI showing the tumor in the nasal cavity and ethmoid; (C) Axial MRI showing the involvement of the ethmoid and the internal wall of the orbit; (D) PET after endonasal resection of the IP (uptake in the medial wall of the maxillary sinus and nasal septum); (E,F) Endoscopic view of the medial maxillectomy (arrow); (G) Endoscopic view after resection of the lamina papyracea, showing the exposed periorbita (arrow) and dissection of the skull base.
View Figure 6
Figure 6: Synchronous squamous cell carcinoma with IP (T3N0M0). (A) CT showing the tumor in the nasal cavity and the involvement of the innerwall of the orbit; (B) Coronal MRI showing the tumor in the nasal cavity and ethmoid; (C) Axial MRI showing the involvement of the ethmoid and the internal wall of the orbit; (D) PET after endonasal resection of the IP (uptake in the medial wall of the maxillary sinus and nasal septum); (E,F) Endoscopic view of the medial maxillectomy (arrow); (G) Endoscopic view after resection of the lamina papyracea, showing the exposed periorbita (arrow) and dissection of the skull base.
View Figure 6
 Figure 7: Metachronous squamous cell carcinoma with IP (T2N0M0) (A, B) CT: Rightmaxillo-ethmoid-frontal occupation is observed; (C, D) MRI showing ethmoid and frontal recess involvement; (E) Postoperative CT (medial maxillectomy, ethmoidectomy, DRAF II-B).
View Figure 7
Figure 7: Metachronous squamous cell carcinoma with IP (T2N0M0) (A, B) CT: Rightmaxillo-ethmoid-frontal occupation is observed; (C, D) MRI showing ethmoid and frontal recess involvement; (E) Postoperative CT (medial maxillectomy, ethmoidectomy, DRAF II-B).
View Figure 7
Table 1: Patients with squamous carcinomas associated with inverted papilloma. View Table 1
Inverted papillomais a benign, locally aggressive tumor that originates from the Schneiderian epithelium that lines the nasal cavity and paranasal sinuses.
It represents between 0.5 to 4% of nasal tumors, and its incidence is 0.6 to 1.5 cases per 100,000 in habitants per year [2].
The incidence of cancer associated with inverted papilloma is variable.
Some factors may lead to suspicion of malignant changes: Bone erosion, absence of inflammatory polyps, increased radius of then eoplastic epithelium/stroma, increased hyperkeratosis, presence of squamous hyperplasia, high mitotic index, low number of eosinophils, and presence of plasma cells.
In a review of several studies [2] they reported that in 11 series they found atypia in 8.8 cases of 958 patients (1.1%), in 9 series they found dysplasia in 9 cases of 454 patients (1.9%) and in 10 they found carcinoma in situ in 15 cases of 494 (3%).
In total, 6.8% had synchronous carcinomas and 3.6% developed meta chronous cancer.
The interval for the development of a metachronous carcinoma was 52 months.
Most were squamous cell carcinomas but there were also adenocarcinomas, mucoepidermoid carcinomas, transitional cell carcinoma, and verrucous carcinoma.
In our series epidermoid carcinomas predominated, a single patient had a verrucous carcinoma.
Miyazaki found in 70 patients, 6 cases of malignancy. The carcinoma was synchronous in 5 and metachronous in one [3].
Two reviews found between 8.9 and 13% malignancy in inverted papilomas [4,5].
Nygren reported 9 cases with carcinoma in situ or invasive carcinoma in 88 patients operated for inverted papiloma [6].
In our study, the rate of carcinoma associated with inverted papiloma was similar to that described by Nygren [6] and Lawson [5].
The IP-associated squamous cell carcinomas that we diagnosed had an advanced T (T4B: 2, T4A: 2, and T3: 2), only one patient had a cancer staged T2 without bone erosion.
Synchronous carcinomas also predominated over metachronousones, and the time elapsed for the appearance of carcinoma after surgery for IP was 6 years in one patient and 5 in another.
The cause of malignant transformation is no known, but it is known that neoplasms that are positive for HPV have an increase in epidermal growth factor receptor (EGFR) and Ki-67.
High levels of EGFR and Ki-67 are associated with early carcinogénesis [7,8].
The mutation of the p53 tumor suppressor gene has also been implicated as a risk factor for malignant transformation in inverted papilloma. An increase in p53 staining has been observed in inverted papilomas with dysplasia, carcinoma in situ, and with carcinoma when compared to normal controls [9].
Mirza, in a review of 2.000 inverted papillomas, found 7.1% synchronous carcinomas and 3.6% metachronous carcinomas. He estimated that 11% of recurrent inverted papillomas can developa metachronous cancer [10].
It is difficult to identify factors that allow predicting which patients may be at higher risk of recurrence or malignant transformation.
Inverted papiloma exeresis with resection of the periosteum and drilling of the bone at the site of tumor implantation is the surgical technique of choice. This technique with complete resection of the tumor would avoid recurrences and the possibility of malignant transformation.
The endonasal approach with endoscopes allows this surgery to be performed with better vision (magnification) and better visualization of the angles than surgeries performed externally.
Studies show similar results between both techniques [11].
In a review of the literature, Lisan, et al. reported a higher rate of recurrences related to advanced stages of the staging proposed by Krouse for inverted papilloma.
Stage III had more recurrences than I and II [12].
Cancer associated with recurrent inverted papilloma has a poor prognosis, similar to that of other rhinosinusal malignancies.
Castelnuovo, et al. [13] reported 9 carcinomas associated with recurrent inverted papilloma. Only 1 of them remained alive without disease. The prognosis was worse in advanced stages (T3/T4), when the tumor had a high degree of differentiation, transcranial surgery (cranio endoscopicre section) was performed, and when there was recurrent disease.
In a systematic review [14] that included 663 patients with IP-associated squamous cell carcinoma, 596 were staged according to the TNM classification. Four hundred thirty-nine (73.7%) were T3/T4.
Of 650 patients with complete data on local, regional or distant recurrence.
155 (23.8%) had recurrence within a mean time of 24.3 months.
In another review and meta-analysis [15] they reported that patients with squamous cell carcinomas not associated with IP had double the risk of mortality than those with carcinomas associated with IP.
In a study [16] they compared 89 patients with primary squamous cell carcinoma with 84 who had a EC associated with IP.
They found a higher proportion of IP-associated EC originating from the sphenoid and frontal sinuses than primary EC.
Overall and specific survival at 5 years and loco-regional recurrence were similar in both groups.
In multivariate analysis, age > 70 years, advanced stage, and positive surgical margins were independent factors that increased the risk of mortality. Primary EC had a higher incidence of distant metastases.
In our study, EC associated with IP that originated in the frontal and sphenoid sinuses also predominated (4/7).
Most had advanced T (T3-T4:6/7), but despite this, local control of the Disease was achieved in three patients during a 5-year follow-up.
The incidence of squamous cell carcinoma found in our study was 11.11% (7 of 63 patients with inverted papilloma).
Two had metachronous cancer and 5 had synchronous carcinomas.
Local control of the Disease was obtained in three patients during a 5-year follow-up.
We believe that the prognosis and treatment of squamous cell carcinoma associated with inverted papiloma is similar to that of rhinosinusal squamous cell carcinomas not associated with inverted papilloma.
The involved paranasal sinus, the site of the affected sinus, and the extent of the carcinoma (T) are factors linked to prognosis.
Treatment should be the same as for squamous cell carcinomas that are not associated with IP.
We do not declare to have conflicts of interest.