Treatment paradigms against cancer have continuously evolved over the years. Having said that, with its prevalence of more than 2 million cases each year, breast cancer represents an urgent global priority [1]. Breast carcinomas accounted for 11.6 % of cancer cases and were the cause of mortality in as many as 6.6 % of women in the world in 2018 [2]. Toxicity and chemoresistance are significant hurdles in conventional chemotherapy and to avoid these issues, a new approach to drug administration, Metronomic Chemotherapy (MC) has emerged [3]. Metronomic chemotherapy involves treatment at regular, close intervals without prolonged breaks at doses considerably less than the Maximum-Tolerated Dose (MTD) [4]. Recently, MC is being used to intensify adjuvant chemotherapy as well as maintenance therapy for high-risk patients in the adjuvant settings [5]. This systematic review focuses on Randomized Controlled Trials (RCT) that involve adjuvant treatment of breast cancer MC in one arm and without it in the other arm. treatment of breast cancer with MC in one arm and without it in the other arm.
To evaluate effectiveness, RCT is the acknowledged standard and is believed to produce the highest quality of evidence [6]. For questions comparing effectiveness of interventions like this, evidence should be generated from RCTs, which if properly designed, executed, and reported has the potential to provide credible and high-quality evidence [7]. Hence, only RCTs as the design of study were considered for this review. A scoping search was performed in Medline and Embase databases which laid to one systematic review studying metronomic chemotherapy in breast cancer patients. However, it did not specifically compare the efficacy of treatment regimens with adjuvant metronomic chemotherapy and without it and had all types of clinical studies in it. The present review exclusively includes RCTs comparing the efficacy of therapies with adjuvant MC or without it. This review will summarize available evidence of using adjuvant MC owing to its potential in achieving better overall response.
In order to make sure that the most relevant literature is identified, a standard systematic review methodology as laid by National Institute for Health Care and Excellence (NICE) was adopted to inform the process. An electronic database search was conducted in Medline (1946 to Mar-2022) and Embase (1974 to Mar-2022). Medline was chosen because of its rich medical literature with more than 26000 medical subject heading terms whereas Embase was chosen because of its focus on drugs and treatments [8] Table 1.
Table 1: PICO of the research question. View Table 1
A facet analysis was performed to identify key components of the question. For each identified facet, index terms, keywords, abbreviations and synonyms were generated as shown in Table 2. To broaden the search, truncation (*) was used so that plural forms of the terms can also be included. Breast neoplasm as a term was employed as exploded MeSH heading to ensure all subtypes of breast cancer are included. Terms in intervention were not exploded as the closest medical heading of "antineoplastic agent" generated thousands of results not relevant to metronomic chemotherapy. Different synonyms of the response rate along with its abbreviation were used to ensure no relevant study is missed. Boolean operator "AND" was used to combine all three facets of the search strategy so that the results include each of these facets. Similarly, the Boolean operator "OR" ensured that the results contain at least one of the keywords from each facet. The Boolean logic increased the specificity and sensitivity of the search results. Since the area of interest was pre-defined, limits of human only and English language were also applied to exclude irrelevant data.
Table 2: Facet analysis of review question. View Table 2
A systematic search of selected databases yielded 120 results. Post removing 29 duplicates, 91 citations were screened. Titles and abstracts of all the identified studies were then screened through Covidence (https://www.covidence.org). Studies found in both databases were excluded as duplicates. Remaining of the studies were screened for inclusion and exclusion criteria as depicted in Table no. 3. Post removing all irrelevant studies, full texts of all the potentially eligible studies were retrieved.
Table 3: Inclusion and exclusion criteria. View Table 3
It was noticed that most of the existing literature had prospective or retrospective observational studies, indicating a gap in literature that needs to be addressed by conducting RCTs. Only 11 studies were selected based on inclusion criteria, out of which 2 could not be retrieved due to unavailability of full texts. 9 studies with RCT as design were shortlisted, from which 6 studies were excluded because of their focus on comparison between metronomic dosing against conventional chemotherapeutic dosing while 1 of them was conference abstract. Two peer-reviewed studies, [9] and [10], ticked all the boxes in inclusion criteria and were selected for this review. Table no. 4 cites the excluded studies along with reason for exclusion while Figure 1 elucidates the entire screening process.
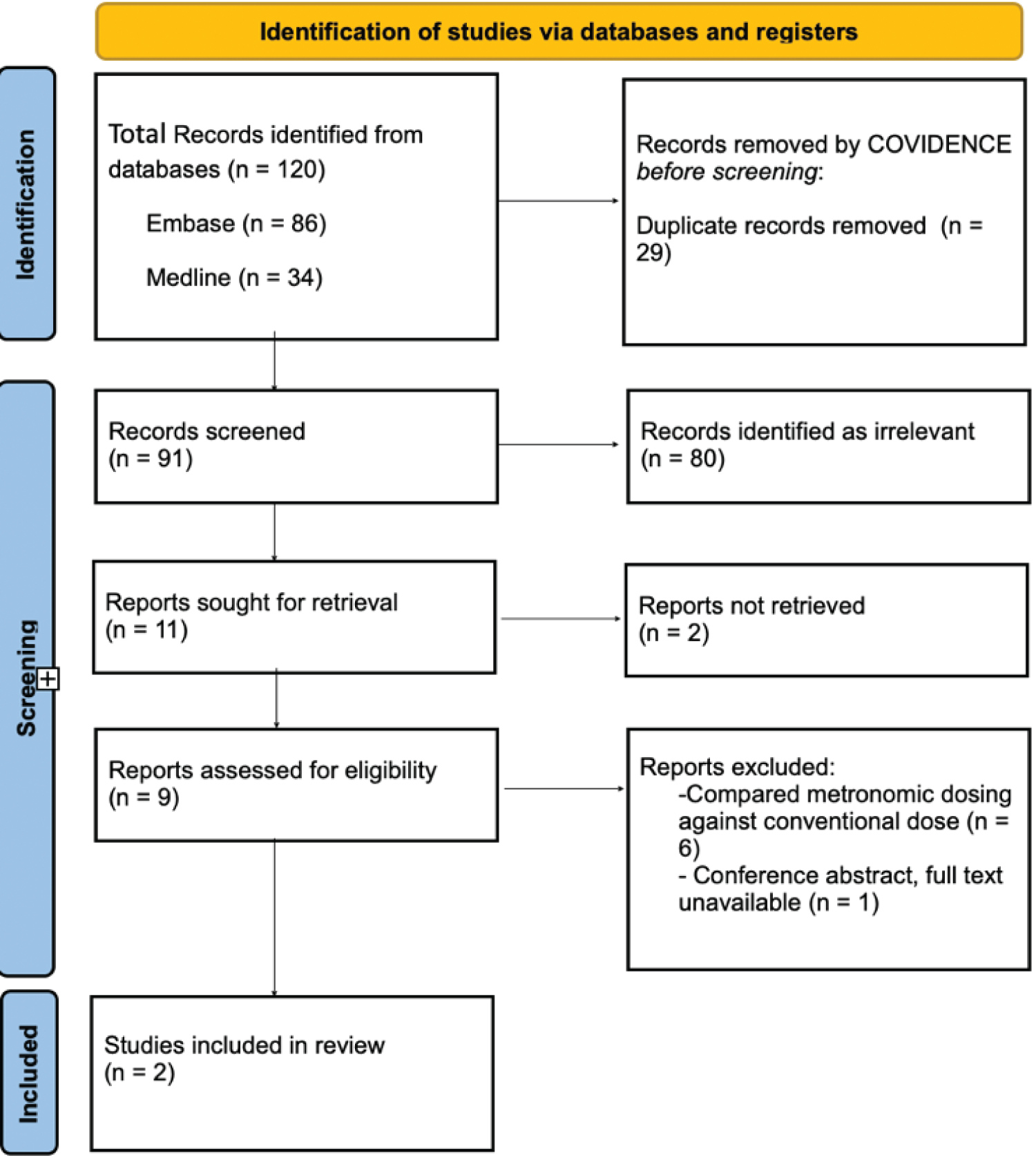 Figure 1: PRISMA flowchart of the screening process.
View Figure 1
Figure 1: PRISMA flowchart of the screening process.
View Figure 1
Table 4: Excluded studies and reasons for exclusion. View Table 4
Wildier, et al. 's study had 80 elderly breast cancer patients while Zhang, et al.'s study had 66 adult breast cancer patients. Even though the study conducted by Wildier, et al. had only elderly patients, the mean age of patients in Zhang, et al.'s study was also in the sixties, indicating little to no difference in patient characteristics, thereby helping to generalize results in adult population. Both the studies were open-label and phase 2 trials with Zhang's study conducted across 30 centres in Europe while Wildier, et al.'s study was single centred. A total of 144 participants from both the studies were analysed on intention-to-treat basis. Both the studies exclusively had metronomic adjuvant chemotherapy with a standard chemotherapeutic drug in one arm with only standard chemotherapeutic drug in another arm. Moreover, use of oral cyclophosphamide as metronomic drug in both the studies made them suitable to compare on same grounds and hence were ideal studies for this review. Both the studies clearly defined overall response rate in the same way and measured it according to Response Evaluation Criteria in Solid Tumors (RECIST) guidelines version 1.1. Table 5 summarizes the features of both studies.
Table 5: Features of studies involved in review. View Table 5
To perform quality assessment and evaluate risk of bias, manual checklist guidelines for RCTs as laid by National Institute for Health and Clinical Excellence (NICE) were followed. Randomization in a trial balances the participant groups about certain confounding and prognostic variables and eliminates selection bias [11]. Wildier, et al. reported a centrally generated randomization technique with minimization method and stratification based on type of breast cancer. Thus, Wildier, et al.'s study certainly had better randomization technique as compared to Zhang, et al.'s study which adopted a simple web-based system without stratification. Lack of proper randomization and allocation concealment put Zheng, et al.'s study at high risk of selection bias despite its patients having fairly uniform baseline characteristics. Wildier, et al.'s study had low risk due to well-designed randomization and stratifying patients based on type of breast cancer.
Blinding helps in minimizing bias and increasing validity of results [12]. Both the studies were open-label and none of the patients, investigators and outcome assessors was masked to treatment. Non-blinded participants who were aware that they were not receiving adjuvant MC may be less likely to comply with trial protocol and more likely to seek additional treatment outside the trial, thereby skewing the findings. However, with an objective outcome such as overall response rate, blinding is least expected to hamper it as the knowledge of allocation would not affect the measurement of tumour response. Moreover, the nature of intervention would have made blinding more difficult. Hence both the studies are considered to possess unclear risk of performance bias.
All 80 participants in Wildier, et al.'s study started intervention but 5 in intervention arm while 3 in comparator arm did not report outcomes to non-measurable disease, leading to per-protocol analysis instead of intention-to-treat analysis. However, a fixed interval of outcome measurement and equal number of participants in both arms at the time of outcome measurement informed the choice of low risk of bias in Wildier, et al.'s study. Zheng, et al.'s study possessed low risk as well due to no loss during follow up along with reported outcomes of all the patients who started the treatments.
Detection bias was judged as low risk in both studies. The decision was influenced by fixed interval of measurement of tumour response in both arms, precisely defined overall response rate and adhering to RECIST version 1.1 guidelines for measuring overall response rate. Both the checklists completed as part of evaluation of risk of bias are attached as Appendix 1 and Appendix 2. Table 6 and Table 7 explore detailed justification of risk of bias and what influenced the decisions for each individual study.
Table 6: Risk of bias assessment of Wildier, et al.'s study. View Table 6
Table 7: Risk of bias assessment of Zhang, et al.'s study. View Table 7
The outcome measure of the studies was the investigator-assessed overall response rate calculated as the sum of complete response and partial response. Even though both the studies are not powered to make direct comparisons in both arms, the findings do show that adjuvant MC can increase the efficacy of overall treatment. Table 8 summarizes the findings of these studies.
Table 8: Findings of included studies. View Table 8
Meta-analysis was performed by pooling data from both studies using RevMan 5.4. Fixed-effect model was adopted considering similar effect sizes and less heterogeneity (Chi-square = 0.23, I square = 0 %). A total of 138 patients (71 in intervention with MC and 67 in comparator) were included in the analysis. The weights were automatically calculated by using sample size and variability within each study. With less heterogeneity and almost identical effect size, both studies carried almost same weightage. A slightly greater weight given to Zhang, et al.'s study indicates findings of this study to provide more information as it is likely to be closer to the true effect, we are trying to determine [13].
The meta-analysis revealed that patients with adjuvant MC are 29 % more likely to have better overall response rate than against with only standard chemotherapy (RR 1.29, 95 % CI 0.95-1.75). A positive risk ratio favouring MC in the forest plot hints at its potential to achieve better overall response. A fairly broad confidence interval can be attributed to small number of pooled studies and smaller sample sizes in these studies. Figure 2 depicts a meta-analysis and forest plot.
 Figure 2: Meta-analysis and forest plot.
View Figure 2
Figure 2: Meta-analysis and forest plot.
View Figure 2
The quality of evidence explored in this review is judged as important as per the GRADE table (Table no. 9) due to consistency in sample size, research design and outcome measurement. The criticality was compromised though due to high risk of selection and performance bias in one of the studies and overall lower sample sizes leading to statistically insignificant results. With no serious inconsistencies, indirectness and imprecision amongst studies, certainty of evidence was adjudged as moderate.
Table 9: GRADE table of evidence (created using https://www.GradePro.com). View Table 9
Breast cancer with its alarmingly high prevalence remains challenging to treat, with certain subtypes of it having no specific targeted therapies until now [5]. Chemotherapeutic agents are often hard to administer over a long period, despite they offer of favourable activity, due to associated side effects or tumor related resistance [14]. Thus, it has become a need of the hour to develop therapeutic strategies that may be deployed over a long time to increase the overall survival rate. Through multiple mechanisms like anti-angiogenesis [15], activation of immunity [16], induction of tumour dormancy [17], and induction of senescence [18], metronomic chemotherapy has shown huge potential in treating cancer and increasing overall response.
This systematic review aimed at summarizing available evidence of adjuvant metronomic chemotherapy and its potential to increase response rate. During literature search, it was realized that very few randomized controlled trials are available that focused on studying the role of adjuvant MC. Many studies have documented evidence of metronomic dosing having better toxicity profiles as compared to standard chemotherapeutic regimens (see Table 5). Since most of the studies were observational, there is a dire need of conducting more RCTs with large sample sizes to find concrete evidence. Both studies included in this review unveil a new paradigm of using MC. Even though the studies in this review did not produce statistically significant results, the comparative clinical benefits of MC in achieving better response against tumours cannot be denied. Thus, a few more well-designed phase 3 trials with large sample sizes may uncover the specific difference and produce statistically and clinically significant results.
This study is the first meta-analysis and review comparing treatment of breast cancer with adjuvant MC and without it. As indicated by the GRADE system of evidence quality rating, the study generated important evidence, forcing us to make a moderate recommendation and suggesting the need for further concrete evidence to corroborate use of adjuvant MC in breast cancer. However, despite its findings, this review had certain critical methodological limitations. With the involvement of second reviewer throughout the entire screening process, the number of relevant studies identified could have been different. Using only 2 databases might have further reduced the number of identified studies and other databases like CINAHL and grey literature would have identified more relevant studies. Since only 2 studies were pooled for meta-analysis, the data might not be enough to prove statistical significance.