Objective: To determine the prevalence of major comorbidities and associated factors among adult diabetic patients attending DM follow-up clinic at selected public hospitals of Addis Ababa, Ethiopia, from April 28 to May 29, 2023.
Materials and methods: Data was collected from April 28 to May 29, 2023. 417 study participants from 4 public hospitals were selected with simple random sampling technique. Data was collected by using structured and pretested questionnaire, medical record was used in order to obtain relevant information’s and measurement was done to obtain BMI. Data was analyzed using SPSS version 25. Bivariable and Multivariable binary logistic regression analysis were done to determine the association between the outcome variable and the independent variables.
Results: The overall prevalence of major comorbidities was 73% at 95% CI (68.7-77.4). The covariates with AOR [95% CI]: age 6.62 [2.10-20.87], residence 2.57 [1.12-5.91], family history of DM 2.85 [1.52-5.37], glycemic control 2.27 [1.04-4.97] and SDSCA score 0.68 [0.47-0.99] were significantly associated with major comorbidities among adult diabetic patients.
Conclusion and recommendation: Age, residence, family history of DM, glycemic control and Summary of Diabetes Self-Care Activities (SDSCA) score were independent predictors of major comorbidities. This reflects that there is a need to give emphasis on interventions targeting the determinants and connotes the need to conduct further research regarding major comorbidities by responsible bodies.
Prevalence, Major comorbidities, Diabetic outpatients, Public hospitals, Addis Ababa, Ethiopia
Diabetes mellitus (DM) is a serious, long-term (“chronic”) condition that occurs when raised levels of blood glucose occur because the body cannot produce any or enough of the hormone insulin or cannot effectively use the insulin it produces [1]. It is a chronic condition where genetic and environmental risk factors act in synergy [2].
DM can be classified into various forms based on the pathologic process, but the vast majority of cases of diabetes fall into two broad categories. In one category, type 1 diabetes, the cause is an absolute deficiency of insulin secretion. In the other, much more prevalent category, type 2 diabetes, the cause is a combination of resistance to insulin action and an inadequate compensatory insulin secretory response [3]. The traditional paradigms of type 2 diabetes occurring only in adults and type 1 diabetes only in children are no longer accurate, as both diseases occur in both age-groups. Children with type one diabetes often present with the hallmark symptoms of polyuria/polydipsia, and approximately half present with diabetic ketoacidosis (DKA) [4]. Symptoms of type 2 DM that may be seen at diagnosis are thirst, polyuria, fatigue and malaise, infections (especially genital candidiasis), and blurred vision [5].
Comorbidity is defined as the presence of at least one or more chronic conditions such as hypertension (HTN), cardiovascular disease (CVD), chronic kidney disease (CKD), tuberculosis (TB), and depression in the same individual. Diabetic comorbidity is defined as the occurrence of one or more chronic conditions in a diabetic patient [6]. The major comorbidities of diabetes are classified as concordant and discordant comorbidities. Diabetes-concordant comorbidities share similar components of pathophysiologic profile and care management as DM (i.e. HTN,CVD,CKD) [7]. Diabetes discordant comorbidities have no direct relationship with diabetes in terms of pathophysiologic profile or care management (i.e. TB, depression) [8-47].
Addis Ababa is the national capital of Ethiopia which is the landlocked country in East Africa. The city is located almost in the center of the nation in the foothills of Mount Entoto about 2,500 m (8,200 ft.) above sea level. Sitting at the foot of Mount Entoto, Addis Ababa is the highest city of Ethiopia. It covers an area of 527 square kilometers. The city has 13 public hospitals [48-50].
The study was conducted in four public hospitals in Addis Ababa. They are Tikur-Anbessa specialized hospital, Yekatit-12 hospital, Menilik-II memorial hospital, and Zewditu memorial hospital.
The study was conducted from April 28 to May 29, 2023.
An institution based cross-sectional study design was used to conduct the study.
All adult diabetic patients who are attending DM follow-up clinics at public hospitals of Addis Ababa, Ethiopia. Participants provided informed consent verbally both in written and spoken way before being interviewed. Data was also accessed from the hospital archive office after obtaining ethical clearance from Addis Ababa city administration health bureau.
Ethical clearance is obtained from Addis Ababa health bureau ethical clearance commitee and submitted to three government hospitals, namely Zewuditu memorial hospital, Minilik II memorial hospital, and Yekatit 12 medical college hospital. Each participant was agreed to participate in the study. Consent to publish, was obtained from each participant.
All eligible adult diabetic patients who are attending DM follow-up clinics during the study period at selected public hospitals of Addis Ababa, Ethiopia.
The sampling procedure used in this study is presented schematically below (Figure 1).
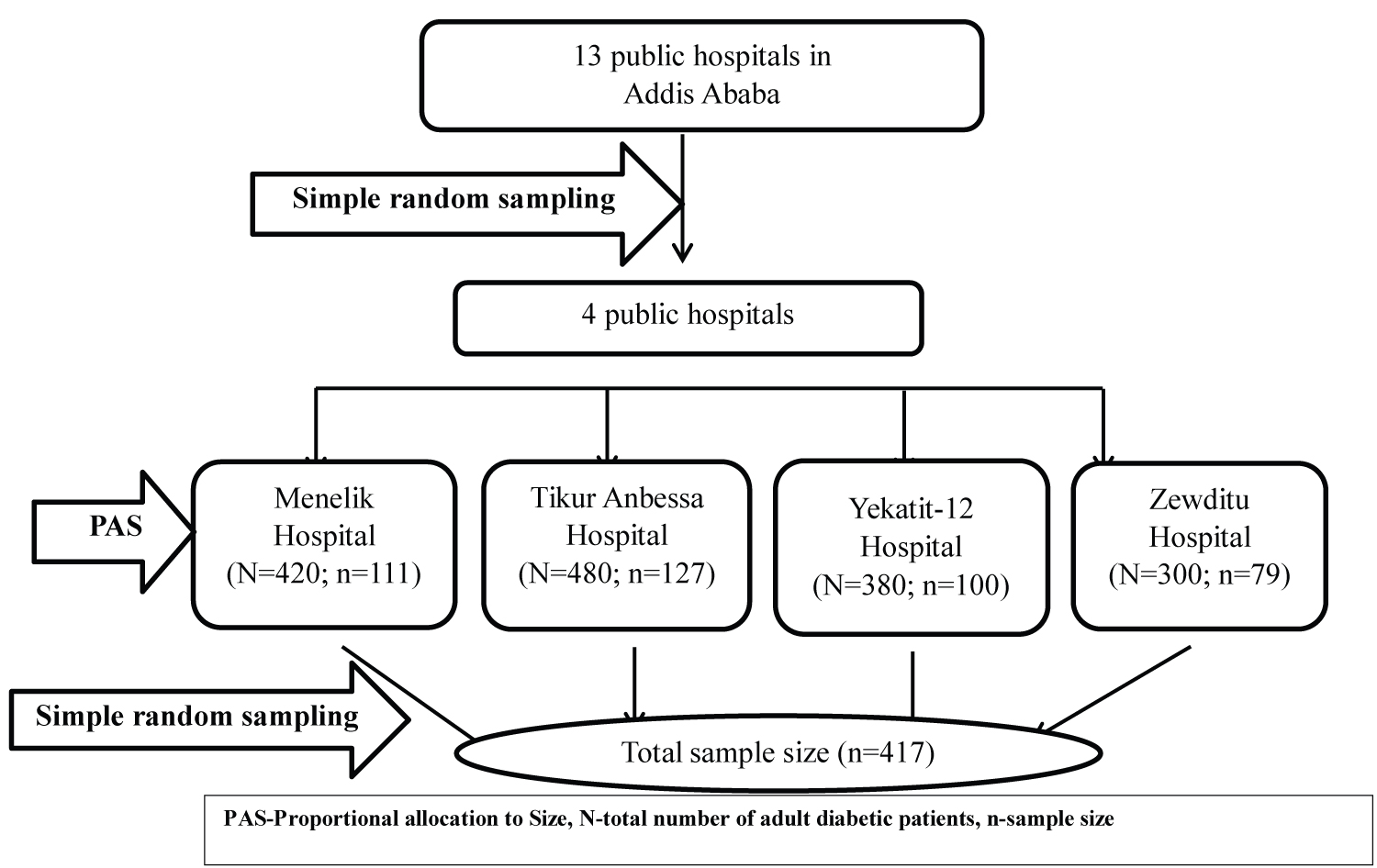 Figure 1: Schematic presentation of sampling procedure for the prevalence of major comorbidities and associated factors among adult diabetic patients attending diabetic follow-up clinic at selected public hospitals of Addis Ababa, Ethiopia, 2023.
View Figure 1
Figure 1: Schematic presentation of sampling procedure for the prevalence of major comorbidities and associated factors among adult diabetic patients attending diabetic follow-up clinic at selected public hospitals of Addis Ababa, Ethiopia, 2023.
View Figure 1
Data was collected by using a pretested interviewer administered structured questionnaire (Amharic version), data extraction form and measurement. The structured questionnaire has four sections. The first section contains socio-demographic characteristics eliciting information on socio-demographic details (age, sex, place of birth, residence, religion, educational level, marital status and monthly income) which is adopted and modified from “Diabetes Comorbidity Evaluation Tool in Primary Care (DCET- PC)” [51]. The second section contains questions regarding lifestyle (physical exercise, alcoholic intake and smoking. The third section contains information regarding diabetic self-care which was elicited using the “Summary of Diabetes Self-Care Activities (SDSCA)” questionnaire, which is adopted from a validated SDSCA measure revised from seven studies result [52]. The SDSCA tool is frequently used to measure the domains of diabetic self-care practices: diet, exercise, blood sugar testing, foot care and medication adherence. Participants were asked to indicate the number of days they were engaged in each of the self-care behaviours for the past 7 days. The overall mean score was calculated by summation of scores of the items in each domain divided by the number of items. After calculating the overall mean score, patients were classified as being above the mean score if patients scored ≥ 3.5 and below the mean score if patients scored < 3.5. To obtain mean SDSCA score, the response to the negatively stated items (items 2 & 6) was reversed (e.g., 0 = 7, 1 = 6, 2 = 5, 3 = 4 & 4 = 3, 5 = 2, 6 = 1, 7 = 0) and then all the other items were summed up. The fourth section which is adopted from a relevant literature contains utilization of health insurance and participants were asked whether they are utilizers of health insurance or not [53-57]. Information regarding presence of major comorbidities and clinical characteristics such as duration of DM and DM treatment, type of DM, family history of DM, type of diabetic drug used and haemoglobin A1c (HbA1c) of the participants were obtained through a review of medical records using a data extraction form. Measurement, of weight in Kg and height in cm, which was then converted to meter, was done to obtain BMI. BMI was calculated as BMI = weight in kg/height in m 2 .
Data was entered in EPI info version 7.2.5 statistical software data which was then exported to SPSS windows version 25 software for further analysis. The outcome variable of this study was major comorbidity. The outcome variable was re-coded to dichotomous outcomes: either the diabetic patients having major comorbidity or not. Binary logistic regression analysis was done. Invariable analyses and crude odds ratio with 95% confidence interval (CI) were used to see the association between independent variables and the outcome variable by using binary logistic regression. Independent variables with p-value of ≤ 0.25 were included in the multivariable analyses to control confounding factors. Adjusted odds ratio (AOR) along with 95% CI was estimated to identify the factors associated with major comorbidities among diabetic patients using multivariable binary logistic regression analysis. Level of statistical significance was declared at P-value ≤ 0.05.
In this study, a total of 397 adult diabetic patients were participated making a response rate of 95.2%. Among the total respondents, 194 (48.9%) were males and 203 (51.1%) were females. The mean age was 51.78 years (SD ± 15.54) and majority of the patients 161 (40.6%) were in 60 and above age category. Most of the participants 253 (63.7%) were married. The result on educational status showed the largest proportion of participants 137 (34.5%) achieved post-secondary education followed by secondary level which accounts 124 (31.2%) (Table 1).
Table 1: Socio-demographic characteristics of study participants at selected public hospitals, Addis Ababa, Ethiopia, 2023 (n = 397). View Table 1
In the current study, most 209 (52.6%) of the respondents had no family history of DM. 269 (67.8%) of participants were diabetic for > 10 years. The mean duration of diabetes was 9.05 years (SD ± 5.77). The mean duration of treatment was 8.78 years (SD ± 5.44). The majority 346 (87.2%) of the DM patients were diagnosed for type 2 DM. Total of 215 (54.2%) of the patients had poor glycemic control and the mean HgbA1C was 7.40 (SD ± 1.11) (Table 2).
Table 2: Clinical characteristics of study participants at selected public hospitals of Addis Ababa, Ethiopia, 2023. (n = 397). View Table 2
Among the study participants 325 (81.9%) do regular physical exercise with most 217 (66.8%) of them having less frequent physical exercise. Regarding alcoholic intake, 122 (30.7%) consumed alcohol and majority 56 (45.9%) of them were frequent alcohol drinkers. Most 37 (62.7%) of participants were mild smokers (Table 3).
Table 3: Lifestyle and behavioral factors among study participants at selected public hospitals of Addis Ababa, Ethiopia, 2023. View Table 3
SDSCA score was computed from 9 question items each having a score of 0 to 7. The overall mean score of participants was calculated by summation of the score of the items divided by the number of question items with 3.5 being the mean cut-off score. Majority 235 (59.2%) of the respondents were below the mean score and 162 (40.8%) were above the mean score. The mean of mean SDSCA score among respondents was 3.33 (SD ± 0.79). The minimum mean score was 1.43 and the maximum was 6.14.
The result regarding the utilization of health insurance showed that most 333 (83.9%) of the study participants were utilizers of health insurance and the rest 64 (16.1%) of the participants were not.
The overall prevalence of major comorbidity among adult diabetic patients attending DM follow-up clinic was 73% at 95% CI (68.7-77.4). The major comorbidities were hypertension (59.7%), dyslipidemia (46.1%) and CVD (22.2%) with IHD (43%), HF (25%) and stroke (32%) followed by CKD (10.8%), cancer (2.5%), asthma (1.8%), and depression (0.5%) (Figure 2). Among patients with comorbidity, 93.1% had concordant comorbidity whereas 32% had one comorbidity (Table 4).
Table 4: Frequency distribution of number and type of comorbidities among diabetic patients with comorbidity attending diabetic follow-up clinic at selected public hospitals of Addis Table Ababa, Ethiopia, 2023. View Table 4
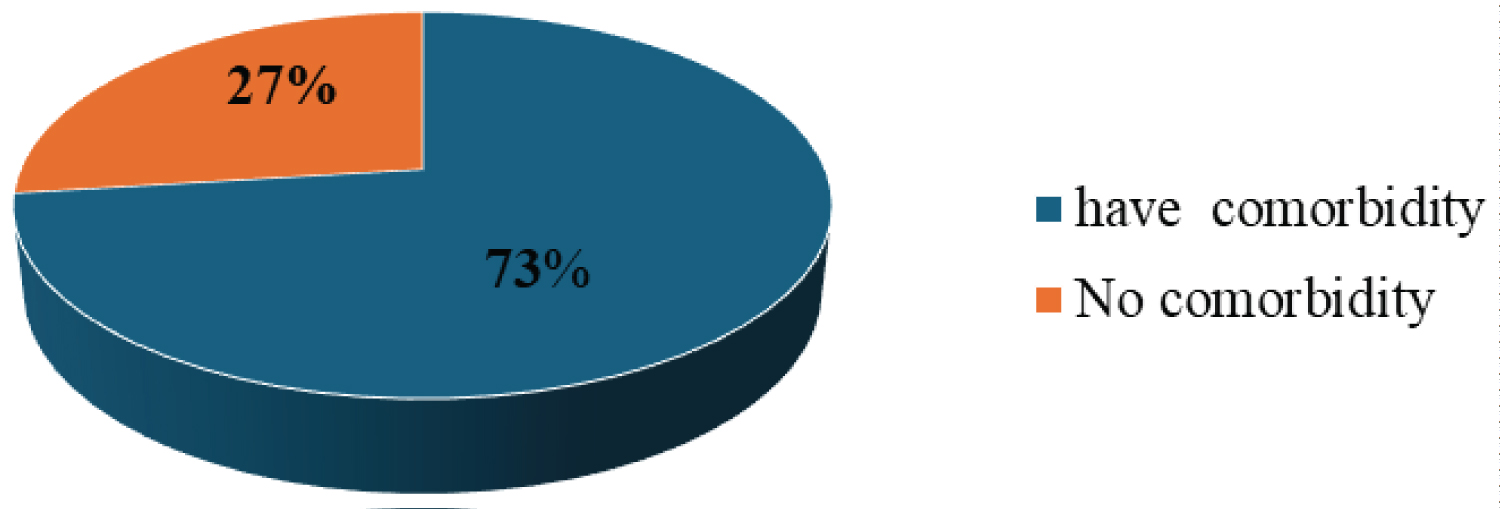 Figure 2: Pie chart description of prevalence of major comorbidities among adult diabetic patients attending diabetic follow-up clinic at selected public hospitals of Addis Ababa, Ethiopia, 2023.
View Figure 2
Figure 2: Pie chart description of prevalence of major comorbidities among adult diabetic patients attending diabetic follow-up clinic at selected public hospitals of Addis Ababa, Ethiopia, 2023.
View Figure 2
Variables with P-value of ≤ 0.25 in the bivariable binary logistic regression analyses were entered to multivariable logistic regression analysis. In bivariable analyses the covariates: age, marital status, employment status, residence, income, type of DM, duration of DM, duration of DM treatment, family history of DM, glycemic control, SDSCA score and utilization of health insurance were associated with major comorbidity. In multivariable analysis, the covariates: age, residence, family history of DM, glycemic control and SDSCA score were statistically significant at 5% level of significance.
The odds of having major comorbidities among adult diabetic out-patients who were 60 or more years old was 6.62 times higher than those in the age group of 18-39 years-old. [AOR = 6.62; 95% CI: 2.10-20.87] (Table 5). Distribution of comorbidity among participants by age category is presented below (Figure 3).
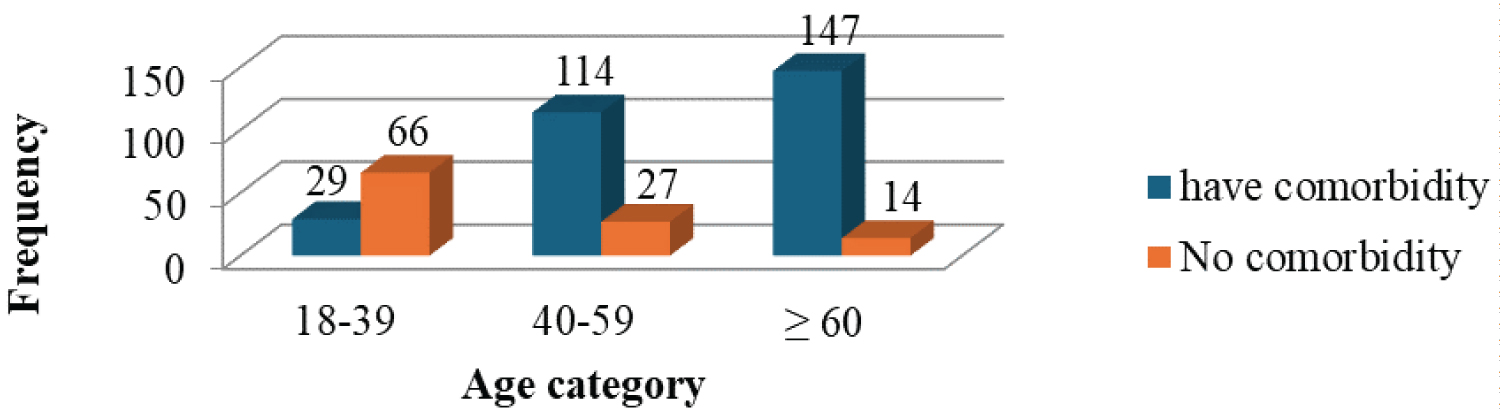 Figure 3: Distribution of comorbidity by age category among adult diabetic patients attending DM follow-up clinic in selected public hospitals of Addis Ababa, Ethiopia, 2023.
View Figure 3
Figure 3: Distribution of comorbidity by age category among adult diabetic patients attending DM follow-up clinic in selected public hospitals of Addis Ababa, Ethiopia, 2023.
View Figure 3
Table 5: Bivariable and multivariable logistic regression analysis of factors associated with major comorbidities among adult diabetic patients attending diabetic follow-up clinic at selected public hospitals of Addis Ababa, Ethiopia, 2023. View Table 5
Moreover, the odds of developing major comorbidities among adult diabetic out-patients living in the urban was 2.57 times higher than those living in the rural [AOR = 2.57; 95% CI: 1.12-5.91] (Table 5). Furthermore, the odds of having major comorbidity among adult diabetic out-patients who had family history of DM was 2.85 times higher than those with no family history of DM [AOR = 2.85; 95% CI: 1.52-5.37]. Likewise, the odds of developing major comorbidities were 2.27 times higher for adult diabetic outpatients with poor glycemic control as compared to those with good glycemic control [AOR = 2.27; 95% CI: 1.04-4.97]. The distribution regarding comorbidity among participants by glycemic control is presented below (Figure 4).
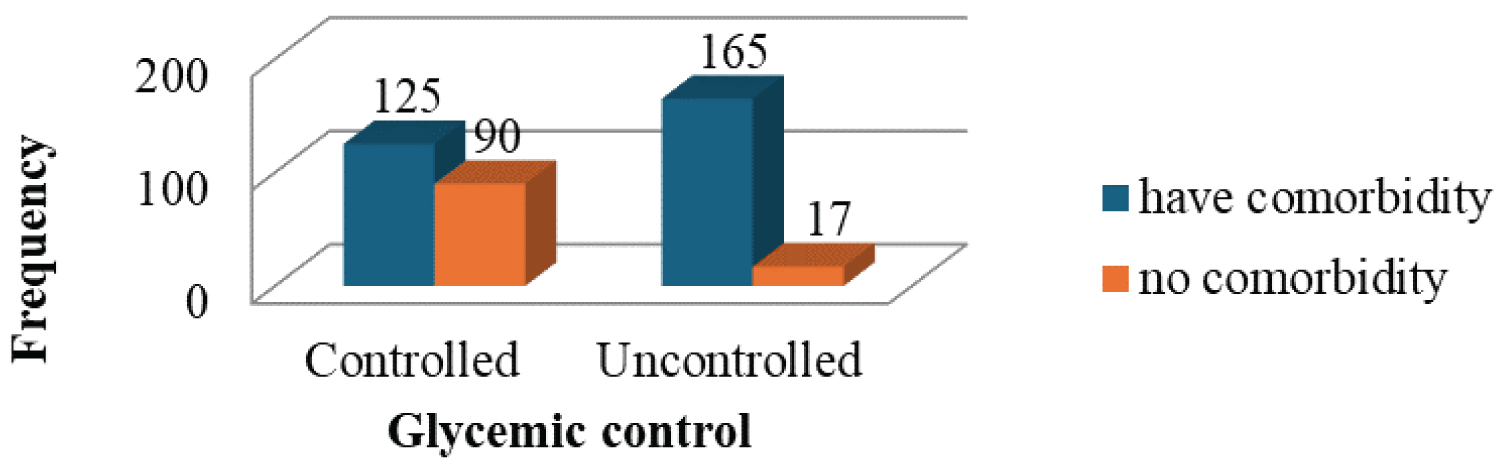 Figure 4: Distribution of comorbidity by glycemic control among adult diabetic patients attending DM follow-up clinic in selected public hospitals of Addis Ababa, Ethiopia, 2023.
View Figure 4
Figure 4: Distribution of comorbidity by glycemic control among adult diabetic patients attending DM follow-up clinic in selected public hospitals of Addis Ababa, Ethiopia, 2023.
View Figure 4
Finally, for each one score increase in the mean SDSCA score, the odds of having major comorbidity decreases by 32% [AOR = 0.68; 95% CI: 0.47-0.99] (Table 6).
Table 6: Bivariable and Multivariable analysis results…Continued. View Table 6
The present study assessed the prevalence of major diabetic comorbidities and its associated factors among adult diabetic patients attending DM follow-up clinic at selected public hospitals of Addis Ababa, Ethiopia. Hospital-based cross-sectional study was conducted. In the present study, the prevalence of major comorbidities among adult diabetic patients was high which is 73% at 95% CI (68.7-77.4). The current result of the prevalence of major comorbidities among adult diabetic patients is comparably lower than the findings of studies conducted in different parts of the world, Spain (82%), Netherlands (84.6%) and China (93.7%) [15,24,58]. In contrast, this study found a higher prevalence as compared to the previous cross-sectional study done in Harar, Ethiopia which was 55.8% [22]. The reason for variation across studies might be due to the difference in the target population, most of the studies used patients with type 2 diabetes, which is different from this study that considered both types of DM. Further, the context of socio-demographic variations and methodologies used might explain the observed differences.
The finding of the current study also showed that adult patients with diabetes mellitus have a high prevalence of major comorbidities, particularly those comorbidities that are concordant with diabetes, such as hypertension, cardiovascular disease, dyslipidemia, and chronic kidney disease. The most prevalent comorbidity was Hypertension (59.7%) followed by dyslipidemia (46.1%) and CVD (22.2%). This finding is in agreement with a study conducted in Nigeria which had shown that the most common comorbidity among DM patients was hypertension (71.6%) [59]. The study in Turkey and sub-Saharan Africa (SSA) revealed that hypertension, dyslipidemia and CVD were the most common comorbidities among diabetic patients [9,47].
Factors associated with major comorbidities among adult DM patients who were on follow-up were assessed as well. Age was one of the identified risk factors that was significantly associated with having major comorbidities among adult diabetic patients attending DM follow-up clinics. The odds of having major comorbidities among adult diabetic out-patients who were 60 or more years old was about 7 times higher than those in the age group of 18-39 years old. Consistent result was reported by Marry, et al. who found that the occurrence of comorbidity increased substantially with age and was present in most people aged 65 years and older [60]. Evidence generated by a study to assess the association of comorbidities with risk factors among diabetic patients revealed that age had a significant association with diabetic comorbidities. The odds of having comorbidities were 7.33 and 20.14 times higher in the age group 60-69 years and 70-79 years, respectively [61]. Moreover, the study that was carried out in German about the development of comorbidities in type two diabetes had shown that there is an increase in the risk of having comorbidities with age as it was most pronounced in the age group 65+ years. people in this age group were almost 2.75 times more likely to have at least one additional comorbidity [62]. The possible justification could be, as age increases serum concentrations of Advanced Glycation End products (AGEs) increases in diabetic people which is associated with increased risk of developing many chronic diseases such as hypertension, heart failure, stroke, CKD and renal failure through increasing oxidative stress and other mechanisms like up regulation of inflammation and cross-linking of collagen and other proteins [63].
Residence was also identified as another factor that is significantly associated with having major comorbidity among adult diabetic patients attending DM follow-up clinic. The odds of developing major comorbidities among urban resident diabetic out-patients was about 3 times higher than those living in the rural. This finding is in line with a study that was conducted in China which noted that diabetic patients residing in rural areas were 0.75 times less likely to have comorbidity compared to those living in urban areas [AOR 0.75, 95% CI 0.59 to 0.95] [24]. The possible reason could be, people who live in urban areas are more exposed to sedentary lifestyle, changes in eating habits, and unhealthy habits such as alcohol consumption, smoking which makes them more exposed for developing comorbidities as compared to those living in rural areas.
The finding of the present study showed that family history of DM is also another significant factor associated with major comorbidity. The odds of having major comorbidity among respondents who had family history of DM was about 3 times higher as compared to those who had no family history of DM. This finding is in line with the study conducted by Tallon, et al. which showed that People with type 1 diabetes who have a family history are more likely to have related comorbidities such as hypertension, dyslipidemia and gastroesophageal reflux disease (GERD) than those without a family history of type 1 diabetes [64]. According to a study conducted by Wang, et al., family history of diabetes in first-degree relatives is independently associated with a rapid decline in estimated glomerular filtration rate (eGFR). Although the underlying mechanisms are unclear, speculations are risk loci of diabetes might also be associated with the risk of kidney disease. However, in addition to having the same genetic background, families share a similar life style and dietary style [65].
The current study also identified that glycemic control is another factor that is significantly associated with developing comorbidities among DM patients. The odds of developing major comorbidities were about 2 times higher for adult diabetic outpatients with poor glycemic control as compared to those with good glycemic control. A consistent finding was reported by a cross-sectional study conducted in harar, hiwot fana specialized university hospital which showed that the odds of developing comorbidity among diabetic patients with poor glycemic control was 4.41 times higher than those with good glycemic control [AOR:4.41, 95% CI: 2.34, 8.32] [22]. The possible justification might be, excess glucose chemically attaches to free amino groups of proteins collagen and other long-lived proteins in blood vessel walls, which, in turn may trap circulating low density lipoprotein (LDL) that promotes the deposition of cholesterol in the intima thus accelerates atherogenesis. Hyperglycemia also increases the osmolality of the extracellular fluid, triggering water to shifts from the intracellular to extracellular space and cause volume expansion and high blood pressure (BP) [66].
SDSCA score was also found to be significantly associated with major comorbidity. For each one score increase in the mean SDSCA score, the odds of having major comorbidity decreases by 32%. This implies that diabetic self-care among adult diabetic out-patients decreases their likelihood of developing major comorbidities. Self-care management is positively correlated with good glycemic control, reduced comorbidities, complications, and improved quality of life in T2DM patients [67]. For instance, physical exercise is one domain of diabetic self-care which plays an important role in the prevention of comorbidities and management of glucose in people with DM. Physical exercise is beneficial with respect to glycemic control (HbA1c-lowering effect), reduction of diabetes-related comorbidities, and cardiovascular risk factors without an increase of adverse events [68]. An exercise intervention of a period of eight weeks at least, can reduce the level of HbA1c by 0.66% in people with DM, even if there is no weight loss [69].
The overall prevalence of major comorbidities among adult diabetic out-patients was high. This reflects that there is a need to give emphasis on major comorbidities among diabetic patients. Age, residence, family history of DM, glycemic control and SDSCA score were significantly associated with major comorbidities among adult diabetic out-patients.
Based on the findings of the study the following recommendations are forwarded for the following organs:
Healthcare professionals:
✣ They should focus on preventing major comorbidities through screening as well as early identification and management of major
✣ They should educate diabetic patients individually about properly applying diabetic self-care activities in order to achieve optimal glycemic control beyond prescribing medications by focusing on diabetic patients who are at increased likelihood of developing major comorbidities like older, living in urban, family history of DM, poor glycemic control.
Diabetic patients
✣ Patients should properly apply all diabetic self-care activities provided by health care providers.
The hospitals:
✣ The hospitals should give emphasis on major comorbidities that are concordant with diabetes especially hypertension, dyslipidemia and cardiovascular disease.
✣ Diabetic self-care should be included in the health education program of the hospital.
Policy makers:
✣ Emphasis should be given on major diabetic comorbidities at policy level.
✣ Policy makers are recommended to develop integrated and comprehensive health care policies and interventions not only focusing on diabetic care but also on the care of major comorbidities, particularly those that are concordant with diabetes (i.e. hypertension, dyslipidemia, CVD and CKD).
Researchers:
✣ Researchers are recommended to conduct prospective cohort studies to withstand the chicken-egg dilemma which is the issue of this study.
✣ Should conduct further studies on prevalence of major DM comorbidities especially on those that are concordant with DM (i.e. hypertension, dyslipidemia, CVD and CKD).
Above all, I praise Almighty God for strengthening me, never set me aside in all my ups and downs, and during my happiness and sorrow times, and despite all other constraints, brought me to this time. My gratitude goes to Africa Medical College for giving me an opportunity to conduct this research. My deepest gratitude also goes to my advisor Mr. Leul Deribe, for his valuable support in the preparation of this thesis and also his engagement with constructive advice, support, valuable comments, guidance and suggestions. My special thanks also extend to the study participants, data collectors and supervisor. The last but not the least, my special thanks extend to my families, for their love and encouragement to accomplish this thesis.
Data used to support the findings of the study are available from the corresponding author at any time on request through mesfinaklilu@yahoo.com.
Haleluya Girma contributed to the concept, design, data collection, analysis of the research, and manuscript write up; Kabtiymer Shiferaw analyzed the data and reviewed the manuscript; Mesfin Aklilu supervised the research.
Not applicable.
Not applicable.
The authors declare that they have no competing interests.