It's been over 2 years since the pandemic started as a result of the coronavirus. There are striking data showing the incidence, mortality, and recoveries as a result of the viral infection. With several preventive measures established by public health policy, the roll-out of COVID-19 vaccines has been one of the best measures to curtail the menace of the COVID-19. However, there are certain impediments enhancing the hesitancy in the uptake of the vaccine in Africa.
A literature search was made using PubMed and Google Scholar using the following keywords "COVID 19 vaccine", "knowledge," "perception," "vaccine uptake," "vaccine acceptance," "vaccine hesitancy". Upon using the inclusion and exclusion criteria, relevant studies were selected to access the acceptance and hesitancy to the COVID-19 vaccine.
There are various contributory factors that decide acceptance or ensure hesitancy among the populace which includes: Age, education, gender, residence, household income, marital status, religion, information source, access to vaccine and vaccine equity, etc. Major concerns, barriers, and motivators about vaccination were highlighted. Existing data was used to show how each factor played role in the acceptance and hesitancy in the COVID-19 vaccine.
This present study identified key factors that influence vaccine confidence, hesitancy, and acceptance in Africa and in turn proffer sustainable solutions that can be used to address these factors. Through a cumulative review of existing data about COVID-19 vaccine knowledge, confidence, acceptance, and hesitancy, we hope to make contributions that would highlight major influencers of vaccine knowledge and percentage in Africa.
COVID-19 Vaccine, Acceptance, Hesitancy, Public health education, Africa
Coronaviruses are a family of viruses that cause mild to moderate upper-respiratory tract illnesses. Six (6) variants of this highly diverse family namely, 229E, NL63, OC43, HKU1, SARS-CoV, and MERS-CoV have been reported to cause mild to severe respiratory tract infections in humans [1]. The novel severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2), the causative infectious agent of the novel coronavirus disease (COVID-19) was first reported from Wuhan city of China in December, 2019 [2]. As of 14:27 GMT, January 19, 2022, there have been 10,585,817 reported cumulative cases of COVID-19 infection, 235,210 deaths, and 9,366,533 recoveries in Africa [3].
Several preventive measures and instituted guidelines (use of alcohol-based hand sanitizers, washing of hands with soap under runny water, and social/physical distancing among others) were put in place by the World Health Organization (WHO) and health policymakers to mitigate the spread of the COVID-19 pandemic [4,5]. Earlier reports [6] have identified the poor adherence to these important preventive guidelines contributing to viral transmission and mortality. The development, approval, and roll-out of COVID-19 vaccines have been one of the best measures to curtail the menace of the COVID-19. However, this is still met with some resistance. Vaccination is a simple, safe, and effective way of fortifying an individual's immune system against infectious diseases [5]. Currently, there are vaccines available for the prevention of many infectious diseases such as cholera, tetanus, chickenpox, smallpox, human papillomavirus, and COVID-19 while others are in pipeline targeted at addressing major public health issues [5,7]. As part of the response to the outbreak of a novel and severe infectious disease, public health experts aim to develop vaccines that would help the body to mimic the pathogenesis of the causative agent and in turn develop immunity in case of an actual infection. This helps to prepare the body immune down to avoid being caught unawares. Child mortality caused by diseases for which vaccines are now available has declined from 5.1 million deaths in 1990 to about 1.8 million deaths in 2017 [8]. However, vaccine uptake and acceptance vary among people and particularly in Africa, where the acceptance level is rather low and Vaccine-Preventable Diseases (VDPs) are still contributors to the annual mortality rate [9].
The propagation of conspiracy theories and misinformation about COVID-19 and the vaccines have contributed to vaccine hesitancy [4]. These and many other underlying factors are suspected to contribute to the low vaccination rate observed among Africans [10]. With the commencement of vaccine roll-out to several countries (although unevenly), there remains the concern that vaccine availability might not be received with enthusiasm for uptake. There have been over 330 million vaccine doses administered for COVID-19 in Africa as of January 8, 2022, at a rate of about 24.7 doses administered per hundred people. A total of 14.79% of the African population are partially vaccinated while only 9.66% of the population is fully vaccinated. Following this trend, it might take about 1,337 days (or by September 2025) to have 70% of Africans vaccinated with 2 doses of COVID-19 vaccine [10].
Why these figures have stayed low is multifaceted and we can take leads from previous factors facilitating vaccine hesitancy to identify the causes. Usually, concerns about vaccine safety and effectiveness are key players in vaccine hesitancy [11]. The abrupt suspension of the AstraZeneca vaccine in some European countries in March 2021 just a few days after the first vaccination campaign started in Africa [12] might have significantly influenced vaccine confidence [13]. An earlier report [13] on the possible effect of the AstraZeneca vaccine suspension on vaccine acceptance identified that news about the reported side-effects of the AstraZeneca vaccine and the decision afterward to suspend the vaccine had negative, cross-national effects on COVID-19 vaccine acceptance.
The role of social media in facilitating the spread of information which could be fact or mere conspiracy theories which are capable of brewing low vaccine confidence and/or hesitancy cannot be overemphasized. Trust and confidence in the government's policy also influence vaccine uptake. Those who do not trust their government from their previous policies or decisions are less likely to be convinced by the same government to take the vaccine. Many citizens of Nigeria complained about the neglect they felt from the inability of the government to provide basic amenities required to survive during the enforced total lockdown and are reluctant against vaccination as directed by the same government [11].
This present review aims to identify key factors that influence vaccine confidence, hesitancy, and acceptance in Africa and in turn proffer sustainable solutions that can be used to address these factors. Through a cumulative review of existing data about COVID-19 vaccine knowledge, confidence, acceptance, and hesitancy in Africa, we hope to make contributions that would highlight major influencers of vaccine knowledge and percentage in Africa.
Literature search was carried out on Google Scholar [14] in December 2021 using the following keywords: "COVID 19 vaccine," "knowledge," "perception," "vaccine uptake," "vaccine acceptance," "vaccine hesitancy," restricting the search only to African countries and PubMed [15] ("COVID-19" OR "COVID-19" [MeSH Terms] OR "COVID-19 Vaccines" OR "COVID-19 Vaccines" [MeSH Terms] OR "COVID-19 vaccine hesitancy" OR "Africa" [MeSH Terms] OR "cross-sectional study" OR "vaccine knowledge" OR "NCOV" OR "2019 NCOV" OR (("coronavirus"[MeSH Terms] OR "coronavirus" OR "COV") AND 2019/11/01[PDAT]: 3000/12/31[PDAT])). Relevant cited references and similar work suggestions on the PubMed webpage were also accessed from the outcome of the literature search. Each African countries rate of vaccine uptake was accessed via the covidvax webpage [10] and evaluated.
Relevant studies focusing on COVID-19 vaccine knowledge, acceptance, willingness, and/or hesitancy in the African population were accessed for eligibility. Exclusion criteria were preprints that are not yet peer-reviewed, studies not related to COVID-19 vaccine knowledge, acceptance, willingness, equity and/or hesitancy, studies not covering African populations, and review articles. Two independent reviewers (EO and OP) independently screened the retrieved articles by titles, abstracts, availability of free full text, and conformity to the inclusion criteria. Full text of studies that met the inclusion criteria was then read and accessed. Relevant studies with no free full text available were also excluded (Figure 1).
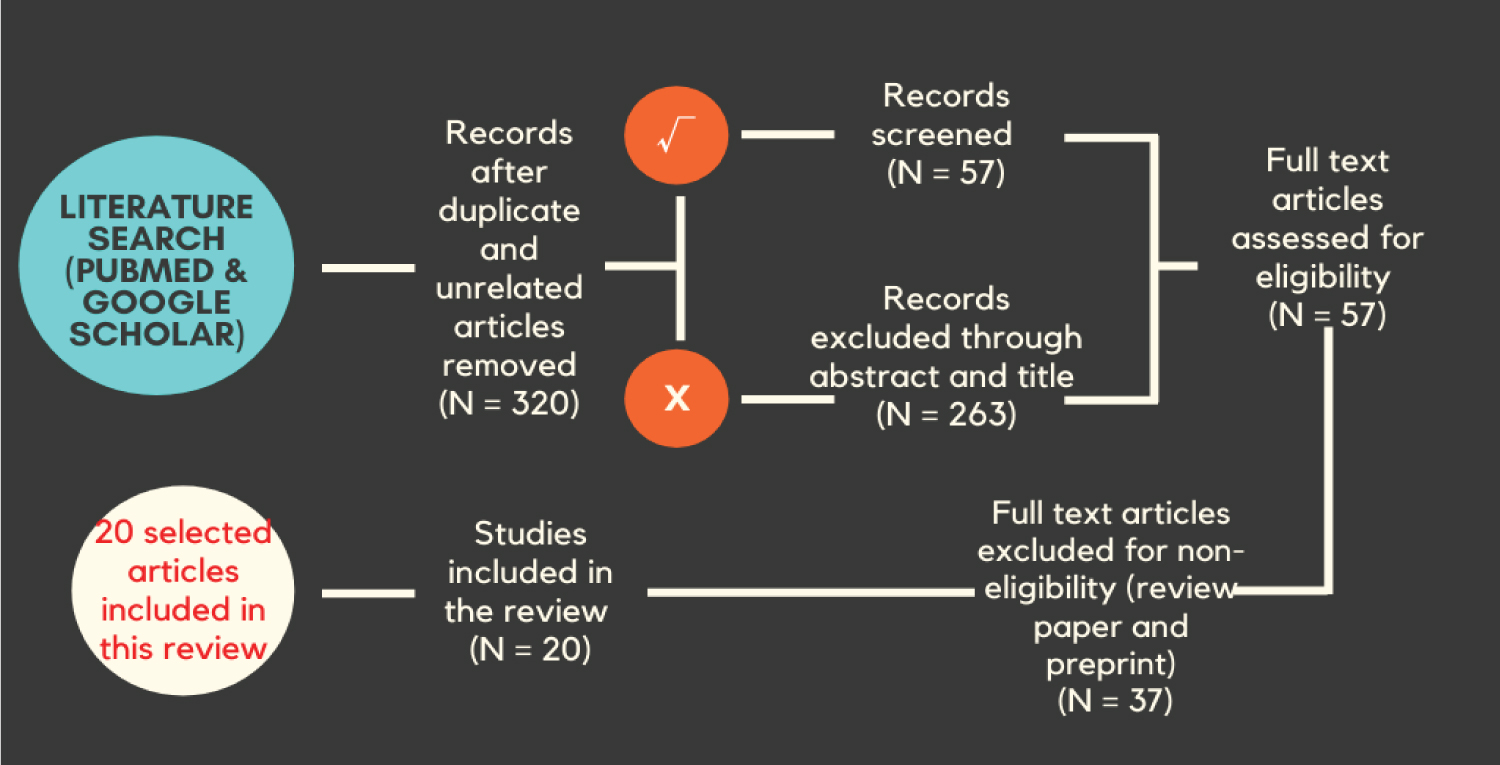 Figure 1: Overview of the search strategy and selection of published articles in the study.
View Figure 1
Figure 1: Overview of the search strategy and selection of published articles in the study.
View Figure 1
The twenty selected articles used for this review utilized either cross-sectional survey (90%) or phone survey (10%) as research instruments with the number of respondents ranging from 200 to 15,699 for a total of 55,625 respondents. The respondents consisted of hospital staff and healthcare workers, medical students, cancer patients, tertiary institution - staff and students, representatives of household, and the general population. The sample population was representative samples from twenty African countries; Burkina Faso, Côte d'Ivoire, Democratic Republic of Congo, Egypt, Ethiopia, Gabon, Ghana, Kenya, Libya, Malawi, Mali, Morocco, Mozambique, Niger, Nigeria, Senegal, South Africa, Sudan, Tunisia, and Uganda.
The following information was extracted from the selected articles for analysis; the time or date the survey was conducted, study location, respondent size and sociodemographic characteristics, the survey instrument used and platform for data collection, outcome accessed, indicator(s) to vaccine uptake or hesitancy and limitation(s) of the study to identify knowledge gap(s) for future studies. We accessed the public database [10] for each country's vaccination rate and projections. Data generated were descriptively summarized and either presented in tables or charts.
Prior to the development and approval of COVID-19 vaccines, adherence to the preventive measures has been pivotal in preventing viral transmission [6]. Since the onset of vaccine roll-out, vaccination has proved to be one of the best measures to curtail the spread and transmission of COVID-19. Although there has been a major debate on its importance, safety, efficacy, and possible future effects, its success is hinged on an individual's willingness and acceptance to be vaccinated [16]. To achieve the WHO vaccination goal, Africa must vaccinate about two-thirds of its population. With the current rate of vaccine uptake and acceptance in the continent, it is projected that two doses of COVID-19 vaccines would be administered to 70% of the African population by October 31, 2024 [10]. This calls for a more concerted effort to mitigate the spread of COVID-19 and needless deaths.
In an Africa CDC study of 15 African countries (Figure 2), respondents' perception about the vaccine and willingness to be vaccinated varied from country to country Green - Those who responded Yes, Blue - No, Yellow - Maybe [17]. Respondents from Ethiopia (94%), Niger (93%), and Tunisia (92%) were more willing to be vaccinated when compared to those from the Democratic Republic of Congo (59%), Senegal (65%), and Gabon (67%). However, Ethiopia and Niger which happened to report the highest percentage of willingness to be vaccinated in the study currently have one of the lowest vaccination rates in the continent (Ethiopia - 7.9% and Niger - 2%). Likewise, the Democratic Republic of Congo which reported the lowest number of respondents willing to be vaccinated (59%) also has one of the lowest vaccination rates (0.30%) in the continent [10]. In contrast, Gabon which reported a low willingness in the report is one of the leading countries in Africa with a moderate vaccination rate (45.9%) [10]. This justifies the major limitation identified in the study that the respondents cannot solely represent all members of the household which may also limit the population-level representativeness of the findings [17]. Although cross-sectional studies can help identify respondents' knowledge, awareness, and perception on a subject, and thereby inform decisions or considerations by policy makers. However, caution must be taken while generalizing findings to the entire population.
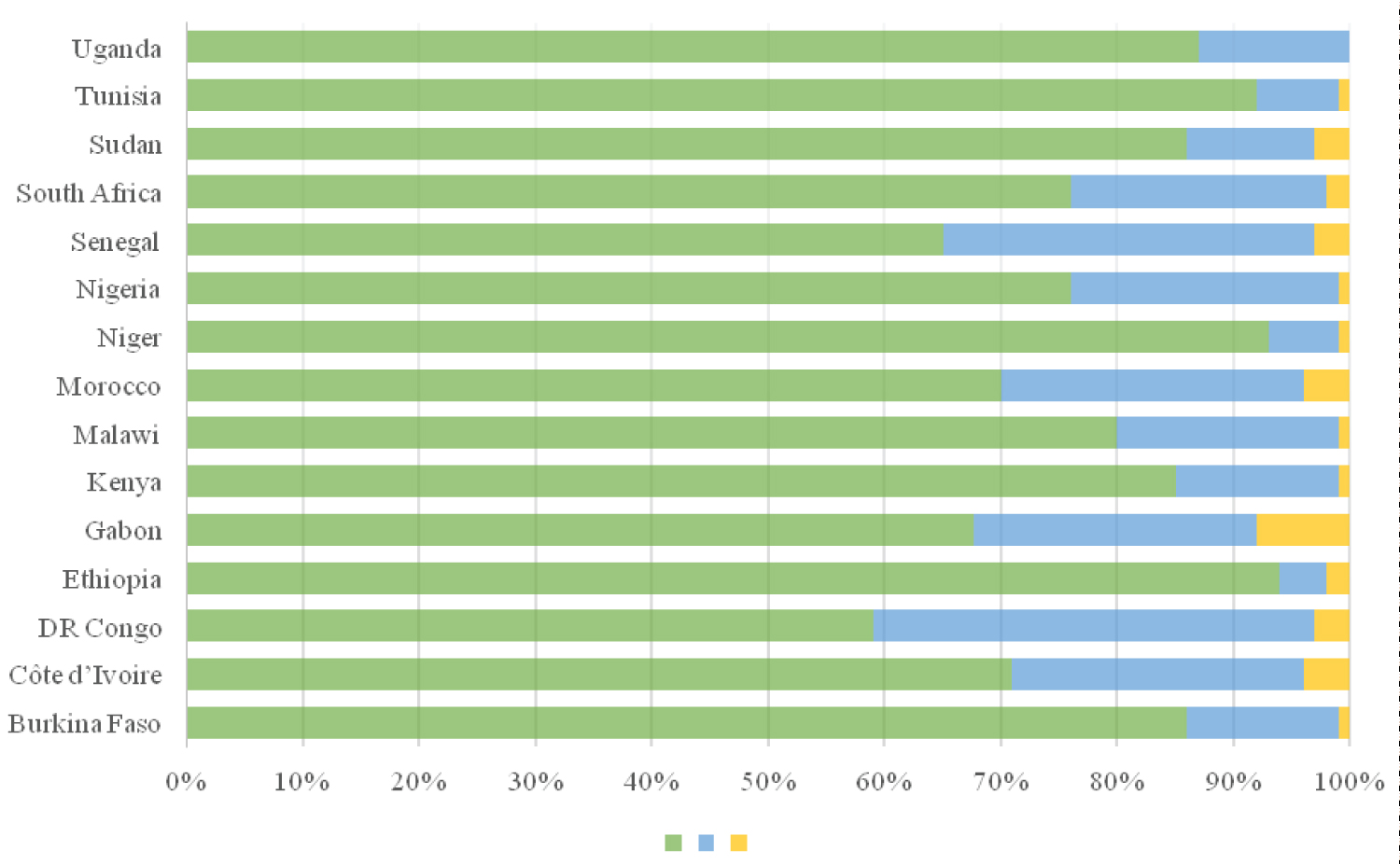 Figure 2: Respondent's willingness to accept the COVID-19 vaccine. Data collated from a study of 15 African countries [17]. Ethiopians sampled reported the highest rate of willingness (94%) while the least was from the Democratic Republic of Congo (59%).
View Figure 2
Figure 2: Respondent's willingness to accept the COVID-19 vaccine. Data collated from a study of 15 African countries [17]. Ethiopians sampled reported the highest rate of willingness (94%) while the least was from the Democratic Republic of Congo (59%).
View Figure 2
In a study of 385 Egyptian healthcare workers [18], none of respondents' age (p = 0.864), governorates (p = 0.602), job (p = 0.237), educational qualification (p = 0.258), working in a COVID-19 isolation hospital (p = 0.599), and being diagnosed for COVID-19 (p = 0.258) were significant factors influencing vaccination decision. Meanwhile, gender and working with COVID-19 patients were notably significant factors (p < 0.001) influencing vaccination decision. We identified other predicting factors that influenced respondents' willingness to be vaccinated.
Age: Respondents' decisions or willingness to accept vaccines is not statistically different according to age [18-20]. Meanwhile, older people are more willing to accept COVID-19 vaccines than younger ones in other reports [5,17,21]. About 43% of older healthcare workers aged 40 years and above were fully vaccinated compared with younger colleagues (30%) aged 18-29 years [22]. COVID-19 infection is more severe in the older population. The higher vulnerability of the older age group to COVID-19 infection might have contributed to their willingness to be vaccinated when compared to younger ones [5].
Among healthcare workers surveyed in Ghana [23], respondents who are 48 years and above were 35 times less likely to recommend COVID-19 vaccine uptake to others (AME = -35, SE = 0.21, p < 0.1) compared to younger colleagues (18-23 years). The same trend was observed in other reports [24] and among Ethiopian healthcare workers [25], where younger ones (less than 30 years) were five times more likely to be reluctant to be vaccinated compared to their older colleagues (40 years and above).
Education: However, willingness to be vaccinated was observed to be lower and less significant in respondents with a higher level of education in Nigeria, Ethiopia, Burkina Faso, and Malawi, this was likewise observed in Mali and Uganda though not significant [19]. Consistent with the earlier report, respondents with lower educational levels tend to be more confident in the safety, importance, and effectiveness of COVID-19 vaccines [17]. Respondents with lower educational levels (up to secondary education) were less likely to be vaccinated [26,27].
In contrast, a study of 496 Nigerians [22] and 1605 Ghanaian [23] healthcare workers identified that being fully vaccinated or willingness to be vaccinated increased with respondents' level of education. Likewise, in a study of Egyptian medical students; senior or graduate students (47%) reported higher vaccine acceptance, while the junior students recorded the highest percentage of hesitancy (50.5%) and refusal (22%) (p = 0.011) [28].
Gender: Acceptance across gender do not differ in Burkina Faso, Malawi, Uganda, and Mali except for Nigeria and Ethiopia where vaccine acceptance by male respondents is statistically significantly higher than female respondents [19]. Similarly, it was observed in a study of 613 healthcare workers [29] where 110 (35.3%) men and 60 (19.9%) women were willing to accept the COVID-19 vaccine and a study of 15 African countries [17], where women tend to be more skeptical about COVID-19 vaccines, even though, they had higher vaccine confidence. This also corroborates other reports on Egyptian [18], South African, [26] and Ghanaian [23,30] healthcare workers where females were less likely to be vaccinated. Male respondents have also shown more willingness to be vaccinated compared to females [31]. While other reports [5] showed no significant relationship between willingness to be vaccinated and gender.
Residence: At a 95% confidence level, higher vaccine acceptance was reported in rural areas in Burkina Faso, Ethiopia, and Malawi [19]. This agrees with a recent report [17] where people who live in rural areas tend to be less reluctant, hence, more willing to accept COVID-19 vaccine compared to those living in cities or urban areas.
Household income: Surprisingly, vaccine acceptance was found lowest among richer households, particularly in Burkina Faso, Uganda, and Nigeria, than those from poor households [19]. While those who are working are more likely to accept COVID-19 vaccines compared to those who are unemployed [17]. Respondent's monthly income was statistically significant as those who earn higher income were more likely to uptake vaccines [27].
Marital status: Marital status greatly influenced respondent's perception of COVID-19 vaccination [OR = 2.06]. Those who were never married were less reluctant than those who are married [5]. This may be due to the dependence of family members for living on those who are married.
Religion: Religious affiliation influenced respondents' perception and willingness to be vaccinated [5]. Even though negligible, religious beliefs (1.43%) were cited as one of the reasons for vaccine hesitancy [5].
Information sources about COVID-19 vaccines: In a study of 15 African countries [17], nearly 2 in 3 (64%) respondents identified television as the most trusted source for information about COVID-19, this was followed by radio (51%), online sources (41%), health bodies (23%), and government sources (18%). Another report [28] identified social media, scientific publications, and healthcare providers as major sources of information about COVID-19.
In a study of 385 Egyptian healthcare workers [18], most respondents (75.06%) stated that they do not get sufficient information about the COVID-19 vaccine, while only 21% trust the information they have about the vaccines. Colleagues, social media, and scientific publications were identified as major sources of information. The decision to be vaccinated by Ethiopian healthcare workers [25] was largely influenced by data or information obtained from either electronic or print media (244, 39.8%). This is rather worrisome as healthcare workers are expected to be one of the first points of contact about health-related concerns. Inability to get satisfying answers from health professionals might have influenced the choice of electronic and print media as the major sources of information.
It is not surprising that most of the study respondents identified electronic or social media as one of the major sources of information about COVID-19 vaccines [18,25,28] which can be attributed to the high internet penetration rate in Africa [32]. The global internet penetration as of January 2021 is 59.5%, meanwhile, Southern Africa has a 62% penetration rate, followed by Northern Africa (56%), Western Africa (42%), Eastern Africa (24%), and Central Africa (26%) [33]. The social media space is a global village where information (both verified and unverified) is disseminated every second. The propagation of misleading information, myths, and conspiracy theories via social media are indeed worrisome as these can influence people's perception, acceptance, and uptake of COVID-19 vaccines [4,5,25]. If not for timely intervention, misinformation peddled on social media indeed frustrated the effort of the Ivorian government to get her citizens vaccinated [34]. This might hold true for many other countries. In a study of 349 Nigerians surveyed in a university community [5], respondents identified the unrestricted recommendation of the use of herbal and orthodox medicines (local spices, chloroquine, and ivermectin) and steam inhalations of leaves on social media as preventive strategies. Social media can however be leveraged to increase awareness on the need for and importance of vaccination.
Access to vaccination and vaccine equity: Vaccine inequity is an unfair distribution of vaccines to nations or people who are in dire need of the vaccine. This includes countries with a high rate of transmission or mortality due to COVID-19, elderly people, frontline healthcare workers, and at-risk groups or those living with co-morbidities [35]. The inequity in vaccine distribution and allocation is taking its toll on at-risk people groups in many low- and middle-income countries (most of which are in Africa) and likewise gives room for the emergence of new variants [36,37]. The efforts of the African Vaccine Acquisition Trust (AVAT) and the COVAX in vaccine supply to Africa have been commendable. However, a lot still needs to be done to achieve the WHO's 70% vaccination target by mid-2022 [35,36]. Vaccine inequity in Africa and other affected regions can be managed by on-scheduled donation as promised by the richest countries, accountability and transparency on the part of vaccine manufacturers, removal of trade barriers or export restrictions that have hindered supply and global architectural plan for pandemic preparedness and vaccine development [36].
Despite the Nigerian government's prioritizing vaccination for frontline healthcare workers, about 68% of healthcare workers in an earlier report in Nigeria reported low ability or difficulty in getting vaccinated [22]. Even though some reports [24,28,38] have shown respondents' willingness to be vaccinated, factors such as vaccine availability, accessibility, affordability (if it has to come at a price), and proximity to vaccination centers might influence people's decision about vaccine uptake [31,39].
As shown in Figure 3, Morocco and Tunisia have been able to vaccinate about 60% of their population, meanwhile, it might still take up to 8,000 more days for the Democratic Republic of Congo to achieve 70 doses per 100 people [10]. This again calls for a more concerted effort by the richest countries to ensure vaccine equity to the low- and middle-income countries [36,37]. Nevertheless, other countries can learn from the remarkable story of Côte d'Ivoire on how to turn vaccine hesitancy into a massive willingness to be vaccinated [34]. As of February 2021, misinformation, mistrust, and vaccine hesitancy frustrated the effort of the government of Côte d'Ivoire to vaccinate its population with the over 500,000 AstraZeneca vaccine doses at her disposal. Despite measures put in place, they were only able to administer 40,153 doses at the end of March 2021. This coincided with the period when the AstraZeneca vaccine was suspended by some European countries due to reported side effects. The government leveraged on additional funding provided by the WHO, consistent dissemination of the right information on the social media space, and engaging leaders - religious, community, and social media influencers. They were able to turn the table from scarcity to a very high demand for vaccines as of September 2021 [34]. The challenge was no longer about vaccine hesitancy or demand but rather vaccine supply [11,37].
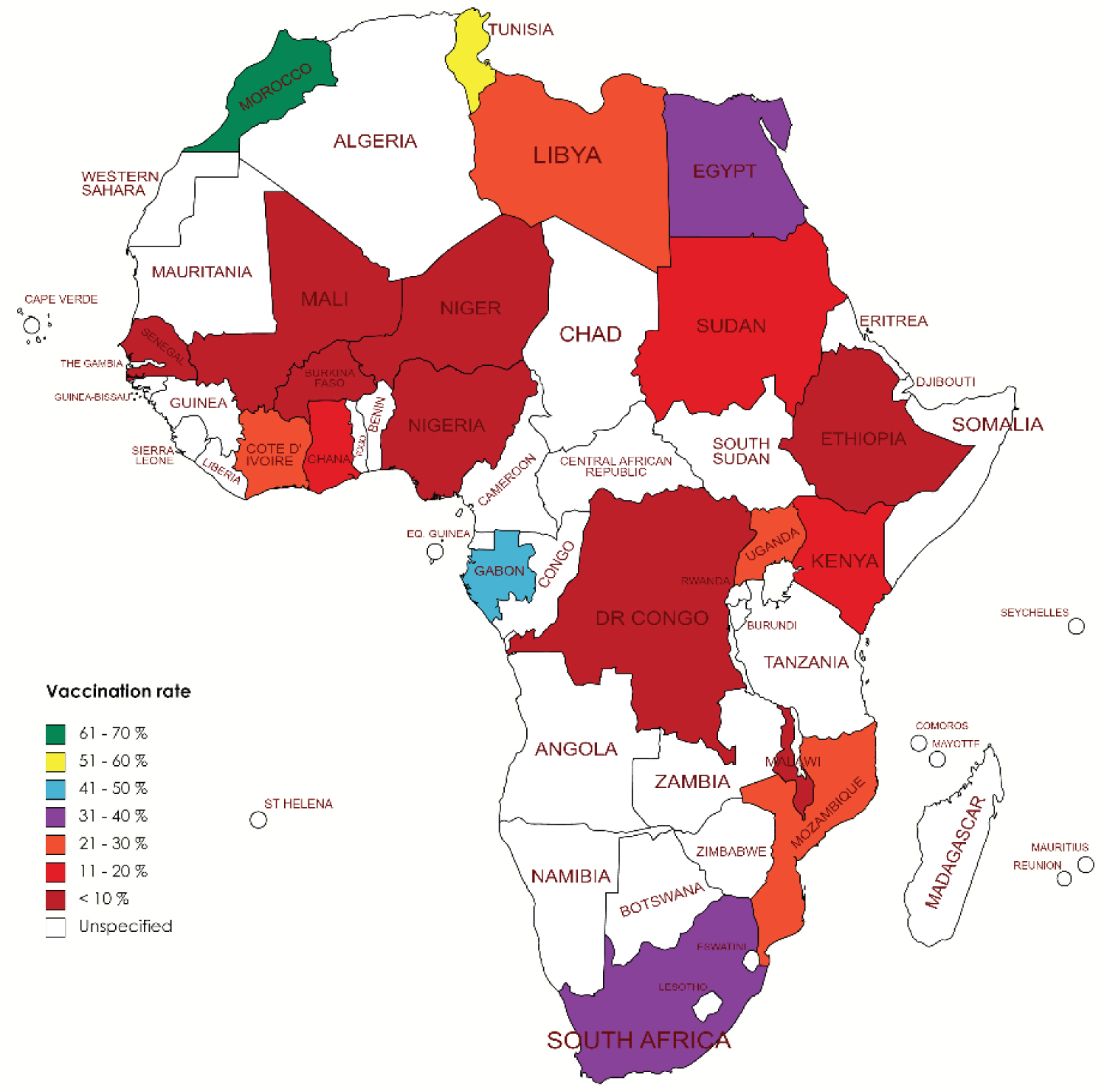 Figure 3: Vaccination rate of African countries reviewed. Morocco had the highest vaccination rate (61.77%) while the Democratic Republic of Congo had the lowest vaccination rate (0.16%) as of January 8, 2022.
View Figure 3
Figure 3: Vaccination rate of African countries reviewed. Morocco had the highest vaccination rate (61.77%) while the Democratic Republic of Congo had the lowest vaccination rate (0.16%) as of January 8, 2022.
View Figure 3
A study [28] on Egyptian students identified that most respondents had concerns regarding vaccine safety, its effectiveness, and adverse effects. Despite good perception about the importance of the vaccine, there still exists hesitancy about the safety, effectiveness, and long-term effects of the vaccine [5,18,20,24,25,30]. Being infected through vaccination was also identified as a concern [25,30]. While non-existence of COVID-19 in Nigeria and no/poor knowledge about the vaccines were also identified by staff and students in a tertiary institution in Nigeria [5]. Healthcare workers who had concerns about vaccine safety had higher chances of vaccine hesitancy [25].
For vaccine acceptance and efficacy, with ≥ 90% efficacy, most respondents 12,006 (79.6%) were willing to take the vaccine, while 9,143 (60.6%) and 6,212 (41.2%) were willing to be vaccinated at the efficacy of ≥ 70% and 50% respectively [38]. Greater vaccine efficacy also influences acceptance [24].
Vaccine's country of produce (23.9%) and specific brand or manufacturers (15.2%) were factors to consider before considering vaccine acceptance [24]. More so, those who had earlier been infected or tested were more likely to be vaccinated [24,27]. The non-existence of COVID-19, intentionally designed as a biological weapon and its side effects were a major concern of 401 Nigerians surveyed [27].
Among healthcare staff and students in South Africa [40,41], most respondents are confident of vaccine effectiveness (97.4%), compatible with their religious beliefs (96.1%), important and safe (95.4%), and are willing to accept the vaccine (89.5%). In contrast, most respondents (74%) among 200 cancer patients surveyed had concerns about vaccine safety and effectiveness and the ability of the health authorities to vaccinate the Tunisian population [42].
Insufficient information about vaccine's adverse effect and the vaccine itself (72.8%) and cost peradventure the vaccine is not free (68%), and mistrust in the vaccination source (55.1%) were major barriers identified by a report on medical students in Egypt [28]. This corroborates another study [21] on health science students in Nigeria where the cost (372, 84.5%) and mistrust in government (324, 73.6%) were major barriers to being vaccinated. Other barriers were refusal to uptake other vaccines in the past [21], vaccine safety and side effects [20], accelerated pace with which the vaccines were developed and produced, fear of possible long-term genetic effects, or implantation of nanochips into recipient via the vaccine [28].
A report on 1,605 Ghanaian health workers [23] identified fear, safety concerns, uncertainty, and religious beliefs as major reasons for unwillingness to uptake the COVID-19 vaccine. Insufficient information about vaccine safety, the efficiency of one's immune system, and not enough vaccine trial were given as major reasons for the non-acceptance [18,31]. This corroborates another study on Ghanaian healthcare workers [30] where vaccine safety and possible side effects were identified as reasons for refusal of vaccine uptake. Unreliability on the results of the clinical trials and efficiency of one's immune system were also major factors for non-acceptance.
A high vaccine hesitancy rate (65.04%) was reported among 349 Nigerians surveyed, even though most respondents (97.13%) are well informed about the vaccine and (121, 34.67%) expressed willingness to be vaccinated [5]. Also, a study from our group found that in Nigeria 33.5% in a 660-population study had confidence in the effectiveness of the vaccine. Reasons include no access to vaccines (31.1%), current health conditions and fear of side effects (19.4%), and insufficient evidence to support vaccine effectiveness or its long-term effect (19.4%) [39]. Surprisingly, most of the respondents have been vaccinated against a disease (78.51%) and have never reported any allergic reaction post-vaccination (85.30%). The major reason for vaccine hesitancy was the concern about vaccine efficacy (34.34%), primarily due to the inability of the vaccine to protect against all SARS-CoV-2 strains and challenges with vaccine storage or preservation at optimal temperature. Others were safety concerns, lack of trust in government and vaccine sources, belief in conspiracy theories, and poor knowledge about the vaccines [5].
The fear of infecting one's family members or getting infected [20].and witnessing confirmed COVID-19 cases were the most reported motivators for vaccine acceptance [28]. Likewise, having an infected friend or family member was positively associated with vaccine uptake [38]. Surprisingly, celebrities' and leaders' advocacy on the COVID-19 vaccine would have no effect on respondents' decision to be vaccinated (69.3%) [18]. While most respondents (over 60%) in another study were willing to be vaccinated if recommended by their healthcare provider or health agencies [40]. The evading risk associated with COVID-19 severity was the most prevalent motivator [18].
Public awareness and assurance of vaccine safety [20,41], first jobs to be taken by political leaders, vaccines to come at no cost, incentives, and free will in deciding whether to take or not were respondent's preferred models to encourage vaccine uptake [27]. A compulsory approach can instill more fear and create avenues for misinformation and conspiracy peddlers about the secret agenda about the COVID-19 and the vaccines [27].
Cancer patients who believed in vaccine safety, efficacy, and effectiveness were significantly associated with willingness to accept the COVID-19 vaccine [42].
The influence of religious and institutional leaders cannot be undermined in low and middle-income countries, as 159 (39.6%) respondents identified they will not be vaccinated if not approved by their religious leaders [27]. While, most health science students in Northwest Nigeria (324, 73.6%) were willing to be vaccinated if recommended by their institutional heads [21].
The insight from this review has highlighted predicting factors like vaccine unavailability, misinformation, and perceived risk or safety concern to be responsible for vaccine hesitancy in Africa. To address these factors, it is important that we acknowledge that peoples' fear and concern are valid, and they should not be coerced into making health choices. Rather, strategic and adequate health education through appropriate mediums should be made to encourage people to make the right health decisions. Almost every new scientific intervention, especially those related to human health, has been faced with some sort of resistance or the other and the reasons have remained relatively the same. For instance, during the re-emergence of the wild poliovirus in northern Nigeria, religious leaders boycotted the national immunization programs due to widespread rumors that the vaccines could be contaminated with anti-fertility agents, HIV, and carcinogens [43]. These and many other similar incidences have shown that the causes of vaccine hesitancy are inherent, and they need to be properly and quickly managed to make the best use of scientific interventions like vaccines. The following two (2) strategies should be considered.
If we want to maximize emergency responses like vaccines during a pandemic, then anti-hesitancy campaigns need to start pre-pandemic. While it is true that no one knows when the next pandemic would be, it is however likely that there would be another pandemic and by then it would be too late to totally curb vaccine hesitancy. Taking cues from the 2009 H1N1 pandemic, it was highlighted that the key to a successful emergency response lies in trust-building and collaboration with community leaders in the preparedness phase [43]. People need to trust science and this trust can be built pre-pandemic and during the preparation stage for intervention. Data about the clinical trial of vaccines should be communicated in clear terms and interpreted for all to understand. A vaccine that is designed for global intervention needs to be understood globally and not only by a fraction of the wealthiest communities if we do not want to keep going in circles. Indeed, the internet has made the world a global village. If rumour peddlers can harness the resources of the media to spread their conspiracy theories, how much more can be done if public health experts can leverage on the internet to improve public health education.
The risk and side effects associated with vaccination are a concern for many people. A survey conducted by the Africa Centre for Disease Control and Prevention (Africa CDC) and the London School of Hygiene & Tropical Medicine across 15 African countries has detailed the need to increase confidence in COVID-19 vaccination on the continent [17]. It surveyed more than 15 000 respondents over August-December 2020 and found that the majority (79%) of the respondents would take the vaccine "if it were deemed safe and effective." An advantage is that vaccine-hesitant individuals, those who are undecided, are different and outnumbers vaccine refusers; therefore, counseling this group might be more effective [44,45].
Almost all medication, treatment, and vaccines carry risks and the reported rare side effects from the COVID-19 vaccine outweigh the risk of being severely infected. There is a concern that the vaccines were developed too quickly. Hence, supporting the conspiracy theory that SARS-CoV-2 was intentionally designed and released. However, prior to the first case of the SARS-CoV-2 infection, much research has been done on similar coronaviruses - SARS and MERS. This contributed to the supposed fast-paced vaccine design, development, and trial [43]. More so, this was a public health challenge that required urgent attention to save humanity. Appreciation to all scientists, frontline health workers, policymakers, the WHO, and government heads, among others who are working tirelessly to put an end to the menace of COVID-19.
From our findings, understanding contextual differences are very important. Cross-sectional studies help to give insight to predicting factors in a local setting. To put a round peg in a round hole, health education is required for all, however, it is important to note that some specific populations might require additional strategies.
No funding was received for the work.
The authors declare no conflict of interest.
Conceptualization: OEO, Data Collation and Analysis: OEO, TO, Draft Writing: OEO, TO, Review and Editing: JOT, AOA, Supervision: OEO, JOT.
1. With several preventive measures established by public health policy, the roll-out of COVID-19 vaccines has been one of the best measures to curtail the menace of the COVID-19. However, there are certain impediments enhancing the hesitancy in the uptakes of the vaccine in various parts of Africa.
2. The insight from this review has highlighted predicting factors like vaccine unavailability, misinformation, and perceived risk or safety concern to be responsible for vaccine hesitancy in Africa.
3. Through a cumulative review of existing data about COVID-19 vaccine knowledge, confidence, acceptance, and hesitancy in Africa, we hope to make contributions that would highlight major influencers of vaccine knowledge and percentage in Africa.