Antiretroviral therapy (ART) suppresses viral reproduction and stop progression of the disease process. Antiretroviral drug adverse reactions negatively influence antiretroviral treatment outcome. Incidence, type and time antiretroviral drug adverse reactions occur is not well documented. The purpose of this study was to investigate time to major antiretroviral drugs adverse reactions and its predictors among patients receiving ART in Hosanna, Ethiopia.
Patients initiated on ART between September 2008 and August 2010 (n = 144) were assessed in a retrospective cohort analysis in Hosanna Hospital in Ethiopia. We used Schoenfeld formula for survival analysis to estimate sample size. We used Kaplan–Meier curve and log-rank test to assess survival time. We used Person-days' time scale to measure time to major antiretroviral drugs adverse reaction. We used Cox regression model to identify predictors of major antiretroviral drugs adverse reactions. We set 95% confidence interval (CI) of hazard ratio (HR) with the corresponding P-value < 0.05 to declare statistical significance. EpI-Data version 3.1 and STATA 10.0 statistical programs used for data processing. We used Mendeley desktop to organize references.
144 participants were followed-up for 1147 Person-days and the incidence rate of major antiretroviral drugs adverse reaction was 48.8 per 1000 person-days. The median time for major adverse drug reactions ± standard deviation (SD) was 15.0 ± 3.7 (CI 7.6, 22.3) days after initiating treatment. The time to major antiretroviral drugs adverse reaction was significantly different for stage of the AIDS disease when patients start ART (Log-rank X2: 9.2; P = 0.02).
High incidence of major antiretroviral drug adverse reactions noted and most of them seen within in 15 days of starting treatment.
ART, Anti-retroviral drug reactions, Survival analysis, HIV/AIDS, Hosanna
ART: Antiretroviral Therapy; CDC: Center for Communicable Disease Control; CI: Confidence Interval; EDHS: Ethiopia Demographic and Health Survey; HIV/AIDS: Human Immune Deficiency Virus/Acquired Immunodeficiency Syndrome; HRs: Hazards ratio; KM: Kaplan-Meier; SD: Standard Deviation; WHO: World Health Organization
Antiretroviral drugs suppress viral reproduction and halt progression of human immune deficiency virus (HIV) disease progress. World health organization (WHO) report shows introduction of ART resulted in significant decline in acquired immunodeficiency syndrome (AIDS) related illness, death and mother to child transmission [1]. The annual number of people dying from AIDS-related causes worldwide is progressively decreasing from 2.2 million in 2005 to an estimated 1.8 million in 2010 [2,3]. Introduction of ART found to have a substantial contribution for reduction of AIDS related deaths. It is known also to prevent and reverse course of opportunistic infections, lessen HIV transmission, restore hope and improve quality of life of AIDS patients [4-6]. Properly taking ART medication is pressing to achieve the needed results of ART.
The eligibility for ante retroviral drugs is established using WHO clinical staging and CD4 count (stage I or II with CD4 count < 350 or Stage IV irrespective of CD4 for adults; CD4 < 25% for children less than 11 months and CD4 less than 20% for children between the ages of 12-35 months). ART is initiated on combination ante retroviral therapy. The combination consisting of nucleoside reverse transcriptase inhibitors, Zidovudine (AZT), Lamivudine (3TC), and Stavudine (d4T)/ 3TC, or Tenofovir (TDF)/3TC in combination with either Nevirapine (NVP) or Efavirenz (EFV) [6-9].
Antiretroviral agents are responsible for a broad range of toxicities, ranging from low-grade intolerances that may be self-limiting to life-threatening side-effects. Like most chronically administered drugs, ante retroviral drugs have documented toxicities and adverse reactions. Ante retroviral drugs adverse reactions range from mild to life threatening effects, but little is known about the time major Ante retroviral drugs adverse reactions in many public health sectors of developing countries including Ethiopia. Antiretroviral drug hostile reactions negatively influence proper adherence to drugs [7,8]. The spectrums of antiretroviral adverse reactions may vary between nations and segment of the population within the same nation [9]. Few side effects seen with in short period of beginning treatment and others appear after long-time use [9].
Condition of patient such as stress, co-morbidity, and multiple drug use significantly associated with adverse drug reactions [10]. Diarrhea, rash, neuropathy and Hepatotoxicity were commonly reported antiretroviral drug reactions [9-15]. There is no study provide information on time to major antiretroviral drugs adverse reactions in Ethiopia. The purpose of this study was to investigate time to major antiretroviral drugs adverse reactions and its predictors among patients receiving ART in Hosanna Hospital, Hosanna, Ethiopia.
We carried out e a retrospective cohort analysis of antiretroviral drug adverse events that were routinely monitored for all patients on ART at Hosanna General Hospital, in Hosanna Town. Hosanna is located 232 km Southwest to Addis Ababa, the capital of Ethiopia and 196 Km west to Hawassa, the capital of Southern regional state of Ethiopia. This Hospital serves over 228 HIV/AIDS patients with support from a USAID funded programs managed by the Ethiopian federal ministry of health. This study was conducted between September 1 2008 and August 30 2010.
The cohort included all patients who were newly initiated on ART between September 1 2008 and August 30 2010 and had at least one follow up visit after initiating treatment. Once eligible for ARVs, all patients were initiated on combination antiretroviral therapy consisting of a nucleoside backbone of Zidovudine (AZT)/Lamivudine (3TC), Stavudine (d4T)/3TC, or Tenofovir (TDF)/3TC in combination with either Nevirapine (NVP) or Efavirenz (EFV).
The adult first line antiretroviral drugs regimen currently used in Ethiopia includes; 1a (d4T + 3TC + NVP), 1b (d4T + 3TC + EFV), 1c (AZT + 3TC + NVP), 1d (AZT+3TC + EFV), 1e (TDF + 3TC + EFV), 1f (TDf + 3TC +NVP), 1g (ABC + 3TC+NVP), and 1h (AZT + 3TC + EFV). The first line antiretroviral drugs regimen for children contains; 4a (d4T + 3TC + NVP), and 4b (d4T + 3TC + EFV). Additionally, 2a (ABC + ddi + LPV/R), and 2b (ABC + ddi + NFV) are the second line antiretroviral drugs regimen for adults. Thereafter, the patient was reviewed monthly for two months.
We used Schoenfeld formula for survival analysis to estimate sample size. We assumed (significance level (α) = 0.05, Power 80%, (β) = 0.8, Zβ = 0.84, Effect size = 0.5, probability of event (major antiretroviral drug adverse reaction) = 0.0.5, proportion of variability among co-variates of interest = 0.5, Square of correlation of independent variables with time to major antiretroviral drug adverse reaction = 0.5) to compute sample size. The final sample size was 144. We used simple random sampling technique (Computer generated random number) to recruit sample records.
We used ADR screening form of WHO to investigate ART adverse reaction. The ADR screening form was designed to identify ADRs that occurred in different organ systems. ADRs were graded on a four point scale using the WHO severity grading. Grade 1 was defined as "transient or mild discomfort; no limitation of activity; no medical intervention/therapy" required; Grade 2 classified as "mild to moderate limitation of activity; some assistance may be needed; no or minimal medical intervention/therapy required"; Grade 3 classified as "marked limitation of activity; some assistance usually required; medical intervention or therapy required; hospitalization possible" and Grade 4 classified as "Extreme limitation of activity; significant assistance required; significant medical intervention/therapy required; hospitalization or hospice care".
The Hospital ART clinic focal person contacted and informed about the details of data collection and ethical considerations. It was agreed that only clinicians working in ART clinic were responsible to contact patients and collect data. We provided two days training for data collectors and supervisors. Data collection tool has two parts. It included baseline demographic and clinical profile and follow-up data of study participants. Drug adverse reactions assessed and recorded every week and other clinical profiles such as CD4 (Cluster Determining cells) and TLC (Total Lymphocyte Count) recorded as scheduled by World Health Organization.
Data entered in to Epi Data and exported to Stata software package for analysis. We used computer assisted data cleaning techniques by data exploration, simple frequency, tabulating for consistency and sorting techniques. Data set was declared to survival-time data by setting time and failure variables. Time from starting treatment until major adverse drug reaction occurred in days set as time variable and Anti-retroviral drug adverse reaction set as failure variable and "1" defines Anti-retroviral drug adverse drug reaction and "0" defines censoring. Kaplan–Meier curves (KM) and log-rank test used to assess survival times. We used Cox regression model to identify predictors of Anti-retroviral drug adverse reactions. Findings presented using 95% CI of HRs with the corresponding P-value. P-value < 0.05 set for significance. We used Epi-Data 3.1 and STATA 8.0 for windows for data processing.
Records lacked data on antiretroviral drugs adverse reaction, time when treatment was started, time when event or censoring were occurred and transferred out were excluded. However, data of patients on both first and second line antiretroviral drug regimen were followed and included in this study.
Institutional review board of strategic information for leadership managing organizations, Addis Ababa University School of Public Health, Ethiopia Public Health Association and Center for Disease control Ethiopia approved this study. Official letter and consent obtained for data collection. One's own identifiers such as name and cell phone numbers removed from data collection tool to find out confidentiality.
We used WHO anti-retroviral drugs adverse effect criteria to define anti-retroviral drugs adverse reactions. Anti-retroviral drugs reactions in grades 2-4 defined as major adverse drug reaction in this study. Operational definition: Time to major antiretroviral drugs adverse reaction: Time from the date of starting ART treatment to major antiretroviral drugs adverse reaction measured in days.
One hundred forty four participants were followed-up for 1147 Person-days. The median age ± SD of participants was 29.6 ± 11.9 years. The mean weight ± SD of participants when initiating treatment was 44.9 ± 13.9 Kg, CI (42.5, 47.2).Similarly, the mean CD4 count ± SD of participants when initiating treatment was 142.2 ± 100.9, CI (88.7, 113.5). Majority (47.2%) of participants started ART at WHO clinical stage three. About 38.2% of participants were TB-co infected. More than ninety percent of study participants received first line ART drugs and large number study participants were taking Zidovudine based regimen. About 47 (32.5%) of study participants changed the ART regimen. The commonly reported reasons for regimen change were developing new TB infection (62.2%), adverse drug reactions (33.8%) and pregnancy (4.0%) (Table 1 and Table 2).
Table 1: Demographic and baseline clinical characteristics of participants. View Table 1
Table 2: Distribution of ADRs by specific characteristics. View Table 2
The mean change in weight ± SD between beginning of the treatment and at the end of 12 months was 3.08 ± 4.10, CI (2.49, 3.77). The mean difference ± SD in CD4 count was 5.38 ± 26.93, CI (0.18, 9.83). The incidence of major antiretroviral drugs adverse reaction was 48.8 per 1000 person-days. The median time to major antiretroviral drug adverse reactions ± SD was 15.0 ± 3.7 (CI 7.6, 22.3) days. Severe anemia (55.7%), skin rash (23.3%), neurotoxicity (16.6%) and Hepatotoxicity (4.4%) were the identified major antiretroviral adverse drug.
The stated time to major antiretroviral drugs adverse reaction was significantly different for WHO clinical stage of patients (Log-rank X2: 9.2; P = 0.02). The KM survival curve at mean of covariates of patients treated for HIV/AIDS in Hosanna Hospital in from September 2008 to August 2010 is steep, rapidly progressing down in the first 40 days after starting of antiretroviral treatment and flat after 40 days. This is the typical feature of short time to event. The nature of KM survival curve shows antiretroviral drug adverse reactions seen with in short period of starting treatment see (Figure 1).
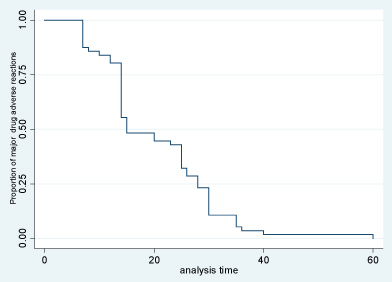 Figure 1: Kaplan-Meier time to event estimate of major antiretroviral drugs adverse reactions.
View Figure 1
Figure 1: Kaplan-Meier time to event estimate of major antiretroviral drugs adverse reactions.
View Figure 1
This study analyzed time to event of major adverse reactions of antiretroviral drugs and its predictors in patients receiving antiretroviral treatment in Hosanna General Hospital. The incidence of major antiretroviral drugs adverse reaction was 48.8 per 1000 person-days of follow-up. The median time for major adverse drug reactions was 15.0 ± 3.7 days after starting treatment. The current finding is in agreement with previous studies reported incidence rate 46.0 per 1000 person-years and most of antiretroviral adverse drug reactions occur within 6 months of starting treatment [16,17]. But, the current finding is greater than study reported to resource-limited setting (incidence of major antiretroviral study 1.64 antiretroviral adverse drug reactions per HIV/AIDS patients receiving ART) [18].
Severe anemia (55.7%), skin rash (23.3%), neurotoxicity (16.6%) and Hepatotoxicity (4.4%) were the identified major antiretroviral drug adverse reactions. Majority of the major adverse antiretroviral reactions seen in the current study were chronic manifestations. However, the median time these manifestations occurred was within the first 15 days after starting treatment. More likely, these differences could be because of the damage of organs by opportunistic infections because of delayed starting of treatment.
Unlike to previous study reported for Nigeria [16], severe anemia took the first rank in the current study. The more likely explanation for the noted difference could be, the combined influence of (long lasting nature of the disease and nutritional status of the users) triggered by known antiretroviral drugs adverse reactions in the current study. Skin rash was the second major antiretroviral drugs adverse reaction in the current study. The finding of the current study supported by previous studies [16,19]. Consistencies in findings suggest skin rash is the common antiretroviral drugs adverse reaction among patients receiving ART in Ethiopia.
Hepatotoxicity found to be the major ART drugs adverse reaction in the current study, which is in line with previous study [20-22]. Habited alcohol use and Hepatitis virus co-infections could cause hepatitis besides ART drugs adverse reactions. The exact reasons for the incidence of identified adverse reactions warrant further study.
In the current study, data extracted from secondary data which is subject to missing important characters such as behavioural factor such as substance use that is an important indicator of time to major adverse reactions. Likewise, records and measurements were undertaken by different individuals risk for introduction of observer bias. Furthermore, we used a small sample that could this all could preclude generalizability of the current study.
The incidence of major antiretroviral drug reaction was high among patients receiving ART. Severe anemia, skin rash, neurotoxicity and Hepatotoxicity were the common antiretroviral drug reaction in Ethiopia. Most of the major antiretroviral drug reactions occur with the first 15 days of initiating treatment. It is worthwhile to monitor major antiretroviral drug reaction with in this period to prevent it and lessen unwanted outcomes.
Institutional review board of Addis Ababa University School of Public Health, Ethiopia Public Health Association and CDC (Center for Disease control of United States of America) approved this study.
Not applicable.
Data will be available from the corresponding author when requested.
The authors declare that they have no competing interests.
CDC funded this study. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
LSA: Conceived and designed the study idea, developed proposal, organized the data collection tool, created data entry template, interpreted findings and wrote the manuscript. FE: Edited the proposal and approved the manuscript. All authors read and approved the final manuscript.
The authors of this study would like to thank Ethiopian Public Health Association, Addis Ababa University, and UNAIDS and Strategic information for leadership training organizing committee for their unreserved technical and financial support. We are also grateful for Hosanna town residents, data collectors and Hosanna town health office for their cooperation during the entire process of data collection.