Ischemic stroke is account for most of the mortality and morbidity cases around the World. Paraoxonase-1 (PON1) is a significant candidate gene for ischemic stroke because of its function against atherosclerosis.
We studied two common polymorphisms (Q192R [rs662] and L55M [rs854560]) of PON1 gene using PCR-based RFLP assay. Overall, 107 patients diagnosed as acute ischemic stroke and 99 healthy controls were enrolled in the present study. We also carried out a meta-analysis containing 3 case-control studies from Turkey.
Allele frequencies of PON1 gene Q192R and L55M polymorphisms didn't demonstrate any significant differences between patients and controls (p > 0.05). However, genotype frequencies were significantly different between patients and controls in terms of Q192R polymorphism (p = 0.030). Statistically significant correlations were observed between systolic and diastolic blood pressures of patients and L55M polymorphism (p = 0.017 and p = 0.039, respectively). Heterozygosity for the both Q192R and L55M polymorphisms demonstrated a statistically significant association with acute ischemic stroke in composite genotype analyses (p = 0.033). The results of meta-analysis showed a significant correlation between acute ischemic stroke and the PON1 gene L55M polymorphism in Turkish population.
PON1 gene Q192R and L55M polymorphisms may have effects on acute ischemic stroke susceptibility in Turkish population.
Acute ischemic stroke, Paraoxonase-1, Q192R, L55M, Genetic susceptibility
AF: Atrial Fibrillation; CT: Computed Tomography; DNA: Deoxyribonucleic Acid; ECG: Electrocardiography; EDTA: Ethylenediaminetetraacetic Acid; HDL: High Density Lipoprotein; HWE: Hardy-Weinberg Equilibrium; LDL: Low Density Lipoprotein; MRI: Magnetic Resonance Imaging; PCR: Polymerase Chain Reaction; PON1: Paraoxonase-1; RFLP: Restriction Fragment Length Polymorphism; SPSS: Statistical Package for the Social Sciences
In worldwide, stroke is the fifth disease that give rise to mortality in individuals between the ages 15-59, and arise to the second order after the age 60 and more [1]. There are several risk factors for stroke, one of which is genetic factors [2]. For this reason, it is significant to characterize gene variants that cause stroke. Ischemic stroke is mostly caused by atherosclerosis, and because of the function of Paraoxonase 1 (PON1) against atherosclerosis, it is a significant candidate gene.
PON1 is localized on chromosome 7q21.3 with the other PON gene family members, PON2 and PON3 [3]. PON1 binds high density lipoprotein (HDL) and prevent low density lipoprotein (LDL) oxidation, which gives it an anti atherogenic activity. PON1 was indicated to have protecting effects towards numerous degenerative and vascular diseases [4-6].
Human PON1 protein comprises 355 amino acids and is encoded by 9 exons [7,8]. PON1 protein concentration and activity are affected by genetic polymorphisms [9]. There are numerous reports from various populations that demonstrate the correlation between PON1 gene polymorphisms and stroke [10,11]. Two frequently observed polymorphisms of PON1 gene are, L55M (163T > A, rs854560) in exon 3 and Q192R (575A > G, rs662) in exon 6 [12,13]. L allele at position 55 was related to increased PON1 function and mRNA amounts and M allele was associated with low stableness of PON1 protein [14]. On the other hand, R allele at position 192 was associated with high-activity plasma paraoxonase and the Q allele specifies a low-activity variant [12].
There are numerous studies investigating the relation between PON1 gene Q192R and L55M polymorphisms and stroke with conflicting results from different ethnic populations, including Turkish population [10,11]. The characteristics of patients were also different in these studies. Because of these conflicting results and the importance of PON1 gene in ischemic stroke, we proposed to investigate if there were associations between PON1 gene Q192R and L55M polymorphisms and acute ischemic stroke in Turkish population.
The study comprised of 99 controls (50 male and 49 female; mean age: 64.22 ± 9.353 years) and 107 patients (68 male and 39 female; mean age: 67.10 ± 12.833 years) admitted to Department of Emergency Medicine in Tokat Gaziosmanpasa University and diagnosed with acute ischemic stroke. Healthy controls that have any cerebrovascular diseases in his or his family were excluded from the study. All patients were examined by emergency physicians and patients, who have focal or global neurological deficit in 24 hours, were suspected to have stroke. Then, these patients were identified if they had ischemic or hemorrhagic stroke by brain computed tomography (CT) or magnetic resonance imaging (MRI). Patients with acute ischemic stroke get involved into the study. Exclusion criterions for patients were: Having cerebral venous thrombosis, brain tumor and other infectious or inflammatory diseases. Patients and controls were compatible in terms of gender and age (p = 0.059 and p = 0.069, respectively). The Institutional Clinical Research Ethics Committee at Tokat Gaziosmanpasa University, Faculty of Medicine was approved the study and written informed consent was supplied from the study population. All the patients were of Turkish origin, from the inner Central Black Sea region of Turkey.
DNA was isolated from EDTA-treated peripheral blood by using a commercial DNA isolation kit. Polymerase chain reaction (PCR) and restriction fragment length polymorphism (RFLP) technics were used to determine the genotypes of PON1 gene Q192R and L55M polymorphisms. The sense 5'-TATTGTTGCTGTGGGACCTGAG-3' and antisense 5'- CACGCTAAA CCCAAATACATCTC-3' primers were used for PON1 Q192R polymorphism. The PCR product of which length was 99 bp was digested into 66 and 33 bp fragments by BspPI (AlwI) in the presence of R allele. The Q allele remained intact. For PON1 L55M polymorphism, the sense5'-GAA GAG TGA TGT ATA GCC CCA G-3' and antisense 5'-TTT AAT CCA GAG CTA ATG AAA GCC-3' primers were used. The PCR product of which length was 170 bp was cut into 126 and 44 bp pieces by NlaIII in the existence of M allele. The L allele remained intact. The 3% agarose gels stained with ethidium bromide were used to analyze the length of fragments under UV Transillumination.
The 'PubMed' and 'Google Academic' internet sites were checked by the aid of the words 'stroke', 'PON1', 'Q192R', 'L55M' and 'Turkish population'. We found 3 reports investigating the correlation between acute ischemic stroke and the PON1 gene Q192R and L55M polymorphisms in Turkish populations, published between 2006 and 2019.
Statistical tests were conducted with Statistical Package for the Social Sciences (IBM SPSS Statistics, version 20) and Open Epi Info software package version 3.01 (www.openepi.com). The Hardy Weinberg equilibrium (HWE) was assessed for each polymorphism. The chi-square and Fisher's exact tests were applied to estimate the HWE and to compare the genotype and allele frequencies between patients and controls. The chi-square test was used to compare parameters between groups. The correlation of Q192R and L55M polymorphisms with clinical and demographic features of patients were determined by us¬ing chi-square, Fisher's exact or analysis of variance (ANOVA) tests. The risk factors were determined by the use of odds ratio (OR) and 95% confidence interval (CI). All p values were 2-tailed and p value < 0.05 was regarded as statistically significant.
Demographical and clinical characteristics of acute ischemic stroke patients evalu¬ated in terms of PON1 gene Q192R and L55M poly¬morphisms were demonstrated in Table 1. Any statistically significant association was not observed between PON1 gene Q192R polymorphism and data of age, systolic blood pressure, diastolic blood pressure, body temper¬ature, respiratory rate, gender, presence of hyperten¬sion and diabetes mellitus, chronic kidney and heart failure, mental status and ECG results of patients (Table 1). However, when we evaluated PON1 gene L55M polymorphism, statistically significant correlations were came up between systolic and diastolic blood pressures and L55M polymorphism (p = 0.017 and p = 0.039, respectively). Both the systolic and diastolic blood pressures were increased in patients with LM and MM genotypes which causes lower PON1 activity.
Allele and genotype frequencies of the PON1 gene Q192R and L55M polymorphisms were demonstrated in Table 2. Any statistically significant diversities were not observed between patients and controls in terms of the allele and genotype frequencies of PON1 gene L55M polymorphisms (p > 0.05) (Table 2). However, not allelic but genotypic distributions were significantly diversity between patients and controls according to Q192R polymorphism (p = 0.030). The frequency of QR+RR genotype was significantly increased in controls than acute stroke patients. Genotype frequency of control group was compatible with HWE according to both polymorphisms. However genotype frequency was not comparable with HWE according to Q192R polymorphism in patient group although, it was comparable with HWE according to L55M polymorphism in the same group (Table 2).
We analyzed the risk related with inheriting the combined genotypes of Q192R and L55M polymorphisms, too (Table 3). Just the heterozygosity for the both Q192R and L55M polymorphisms showed a statistically significant differences between patients and controls (p = 0.033). So, participants that were both QR heterozygote and LM heterozygote have a decreased risk for demonstrating acute ischemic stroke.
The features of population studies investigating the correlation between PON1 gene Q192R and L55M polymorphisms and acute ischemic stroke performed by the present study and other studies from Turkish populations are demonstrated in Table 4 and Table 5, respectively. Figure 1 and Figure 2 show the Forest plot of polymorphisms Q192R and L55M, respectively. According to forest plot, ranges without 1 are statistically significant. So, distribution of QQ : QR+RR and Q : R with Aydin, et al. and QQ : QR+RR with the present study are significant for Q192R polymorphism (Figure 1). The distribution of LL+LM : MM with Aydin, et al. and LL+LM : MM and L : M with the total studies are significant for L55M polymorphism (Figure 2). In terms of the outcomes of the present meta-analysis containing 344 Turkish acute ischemic stroke patients and 288 controls from 3 studies, a statistically significant relationship was found between PON1 gene L55M polymorphism and acute ischemic stroke in Turkish populations (Table 5). The distributions of M allele and MM homozygous genotype was observed to be significantly diverse between acute ischemic stroke patients and controls (L vs. M: OR = 1.309, 95% CI = 1.044-1.642, p = 0.019; MM vs. LL+LM: OR = 1.762, 95% CI = 1.166-2.662, p = 0.007).
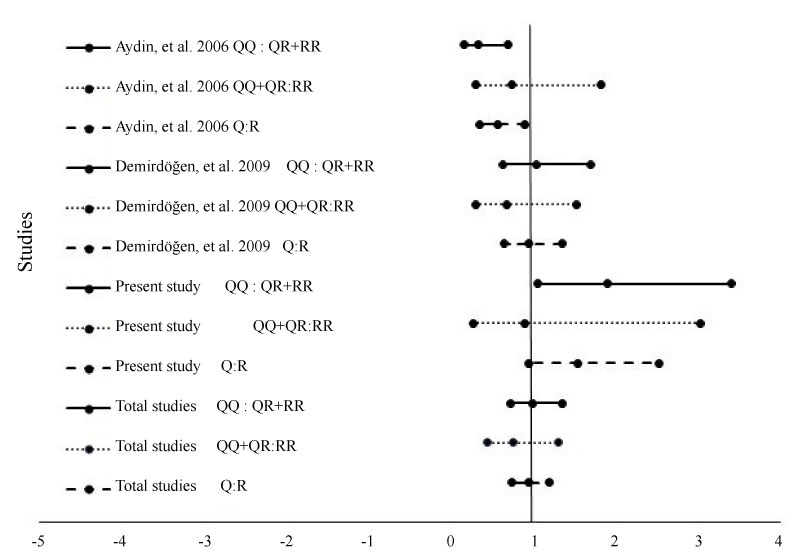 Figure 1: Forest plot of polymorphism Q192R.
View Figure 1
Figure 1: Forest plot of polymorphism Q192R.
View Figure 1
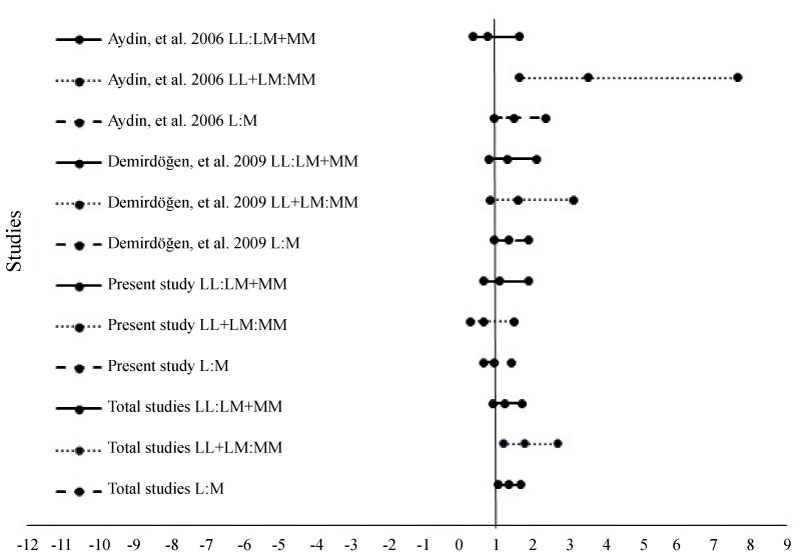 Figure 2: Forest plot of polymorphism L55 M.
View Figure 2
Figure 2: Forest plot of polymorphism L55 M.
View Figure 2
Table 1: Demographic and clinical characteristics of acute stroke patients evaluated according to PON1 gene Q192R and L55M polymorphisms. View Table 1
Table 2: Genotype and allele frequencies of PON1 gene polymorphisms in acute stroke patients and healthy controls. View Table 2
Table 3: Comparative analysis of combined genotypes of acute stroke patients and healthy controls. View Table 3
Table 4: Characteristics of the individual and total studies examined the association between acute ischemic stroke and PON1 gene Q192R polymorphism in Turkish population. View Table 4
Table 5: Characteristics of the individual and total studies examined the association between acute ischemic stroke and PON1 gene L55M polymorphism in Turkish population. View Table 5
PON1 has an antioxidant action against lipid peroxidation caused by free radicals on cell surfaces and lipoproteins [15]. It is a calcium-dependent antioxidant glycoprotein mostly carried on HDL in serum and tissues [16]. It metabolizes many kinds of molecules, and has a large effect on the antioxidant and anti-inflammatory function of HDL to prevent LDL oxidation [17,18]. Because of the ability of reducing the atherosclerosis process, PON1 is one of the most decisive agent in atherosclerosis and in the sequel ischemic stroke.
Polymorphisms in the coding regions of PON1 gene can affect its plasma level, on account of this, it can determine people's susceptibility to ischemic stroke. The most prevalent variant in the PON1 gene is 575A > G which cause Q192R at the protein level. The RR genotype is firmly binds to HDL-apoA-I, while QQ and QR genotypes are associated with free PON1 (18-46%) [19]. For, individuals carrying R allele at position 192 reported to have an elevated PON1-hydrolyzing function than those carrying Q allele [12]. The other frequent variant on PON1 gene is 163T > A which causes L55M at the protein level. PON1 L55M has been demonstrated to directly influence PON1 amounts and function via interaction with the C-107 promoter polymorphism [20,21]. L allele at position 55 was related to increased PON1 function and mRNA amounts and M allele was associated with low stableness of PON1 protein [14].
In the current study, we analyzed the correlation between PON1 gene polymorphisms (Q192R and L55M)and the risk of acute ischemic stroke. In the present study, in terms of genotypes of Q192R polymorphism, we observed that the frequencies of QR+RR genotypes were increased in controls than in patients. In the light of these results, we could comment that individuals carrying QR+RR genotypes could be protected from stroke. Our outcomes are opposite to the outcomes of previous studies. In a recent year, a wide meta-analysis related to PON1 gene Q192R polymorphism and ischemic stroke was published [11]. As regards to outcomes of this meta-analysis containing 38 studies compose of 9022 cases and 9792 controls, increased risk of ischemic stroke was correlated with recessive (RR versus QQ+QR) and allelic (R versus Q) models (OR = 1.15 and OR = 1.14, respectively). Subgroup analysis demonstrated that dominant (QR+RR versus QQ), recessive and allelic models of PON1 Q192R were significantly correlated with ischemic stroke in Asians (OR = 0.81, OR = 1.16 and OR = 1.15, respectively). However, only the allelic model was correlated with ischemic stroke in Caucasians in which Turkish population was also included (OR = 1.10).
For the PON1 gene L55M polymorphism, there was a recent meta-analysis which investigated 14 studies; 2 of these were from Turkey and included 6374 ischemic stroke patients and 12150 controls [10]. According to the results of this meta-analysis, in all populations, no association was observed between PON1 gene L55M polymorphism and ischemic stroke in dominant, and recessive models as our results. Furthermore, any association was not observed between L55M polymorphism and ischemic stroke in Asian or Caucasian populations, either.
There were two more meta-analyses that were published earlier and analyzed the correlation between ischemic stroke and both the PON1 Q192R and L55M polymorphisms [22,23]. Firstly, in the meta-analysis of Banerjee, totally 10 studies (1,484 cases and 4,075 controls) for L55M polymorphism and 11 studies (1,726 cases and 4,379 controls) for Q192R polymorphism were analyzed [22]. According to the outcomes of this meta-analysis, although any significant correlation was not observed between L allele at position 55 and stroke as our results (P = 0.29), the R allele at position 192 demonstrated a meaningful risk for stroke in total study population [OR = 1.25, 95% CI (1.07, 1.46), P = 0.006]. The association of the R allele at position 192 keep going significant in the subgroup of Caucasian subjects, but not in the East Asian population. For this reason, the findings of this meta-analysis showed that Q192R polymorphism could be a significant risk factor for stroke, particularly in Caucasian population. Although Banaerjee indicated R allele at position 192 as a risk factor for ischemic stroke, conversely we observed QR+RR genotypes as a protective factor against ischemic stroke [22].
Secondly Dahabreh, et al. identified 22 studies (7384 cases and 11,074 controls) for Q192R polymorphism, resulted an OR of 1.10 for R allele (95% CI, 1.04-1.17) [23]. For L55M polymorphism, 16 studies (5518 cases and 8951 controls) resulted an OR of 0.97 for L allele (95% CI, 0.90-1.04). For both polymorphisms, results of dominant and recessive models showed the similar effects as allele-based comparisons. Subgroup analyses also demonstrated same findings. As a result of this meta-analysis, PON1 Q192R was correlated with a little raise in the risk of ischemic stroke opposite to our results.
There were three studies investigating the correlation between PON1 gene Q192R and L55M polymorphisms and ischemic stroke in Turkish population [24-26]. According to the results of the study of Aydin, et al. the distributions of QQ and MM genotypes were observed to be significantly increased in controls than in patients [24]. Conversely, the distributions of R allele at positon 192 and L allele at position 55 were meaningfully more frequent in patients than controls. These results are opposite to our results. We observed in the present study that QR+RR genotype frequencies were more common in control group than patient group. According to study of Aydin, et al. the distribution of combined genotype of RR/LL was meaningfully increased in cardioembolic group than in atherothrombotic group [24]. We didn't make such a classification within patient group, but we found that QR/LM composite genotypes were more frequent in control group than patient group. In another study, Can Demirdöğen, et al. investigated 108 ischemic stroke patients and 78 controls [25]. They found that, although it was not statistically significant, the frequency of RR genotype was higher in stroke patients (16.7%) than controls (9.0%, P = 0.129). Also these results were opposite to our results. When they performed composite genotype analyses, they didn't observed any diversities between patients and controls. However the frequency of QR/LM composite genotypes were increased in controls composed to patients (25.6% versus 19.4%) in harmony with our results. The same study group published another report with increasing the number of study population as 172 acute ischemic stroke patients and 105 controls [26]. This time they didn't find the same association although they increased the study population.
When we evaluated PON1 gene L55M polymorphism with clinical characteristics of patients, statistically significant correlations were found between systolic and diastolic blood pressures and L55M polymorphism (p = 0.017 and p = 0.039, respectively). In a recent study, although any significant association was not observed with L allele at position 55, a relation was found between systolic blood pressure and R allele at position 192 (p = 0.004) [27].
The reality that the correlation between PON1 gene Q192R and L55M polymorphisms and acute ischemic stroke shows wide ethnic diversities, and the studies performed in Turkey with partly little study populations resulted in different outcomes, direct us to make a meta-analysis containing the present study and other studies made with Turkish population. We eliminated the study of Can Demirdöğen, et al. because of the same study population with Demirdöğen, et al. [25,26]. In terms of the outcomes of this meta-analysis containing 344 Turkish acute ischemic patients and 288 controls from 3 studies, any correlation was not found between the PON1 gene Q192R polymorphism and acute ischemic stroke in Turkish population. The association that we found in our study was disappeared. However, a new association was appeared, a statistically significant correlation was observed between L55M polymorphism and acute ischemic stroke. The distributions of M allele and MM homozygous genotype was observed to be significantly diversity between acute ischemic stroke patients and controls.
In conclusion, although we found a statistically significant correlation between PON1 gene Q192R polymorphism and acute ischemic stroke, we did not observe any correlation between L55M polymorphism and acute ischemic stroke in the present study. Statistically significant correlations were observed between systolic and diastolic blood pressures of patients and L55M polymorphism. When we carried out a meta-analysis containing 3 case-control studies made in Turkey, the correlation between Q192R polymorphism and acute ischemic stroke disappeared, however a new association was appeared and a significant correlation was found between acute ischemic stroke and the PON1 gene L55M polymorphism in Turkish population. These results show that sample size and ethnic population are the main factors that influence the results of case-control studies.
We obtained ethical approval from The Institutional Clinical Research Ethics Committee at Tokat Gaziosmanpasa University, Faculty of Medicine, reference number 13-KAEK-037.
The authors for the study: "Importance of genetic polymorphisms (rs662 and rs854560) of the Paraoxonase-1 gene as risk factor for acute ischemic stroke in Turkish population" listed on the title page and below have all reviewed and approved the submitted version of this article for publication. This article has not been published or submitted for publishing in any other journal. The content contained in this submission does not require any special permission from other journals or authors.
All data generated or analysed during this study are available from the corresponding author on reasonable request.
The authors declare that they have no competing interests.
NK, NB and SY: conceived and design the study. NB and AK: collected the samples from subjects. PC and TC: performed laboratory experiments. NK and OD: data integration, statistical analyses, and its interpretation. NK and SY: write the manuscript.