Vietnam is one of the countries at high alert of antibiotic resistance. This study aimed to evaluate the antimicrobial susceptibility of P. aeruginosa isolates collected from a Vietnamese hospital in 2019.
A retrospective review was conducted of all reports of P. aeruginosa isolates from the records of the laboratory of Nhan Dan Gia Dinh Hospital between January 01 2019 to December 31 2019.
Of 224 samples, the most common infection from which P. aeruginosa was isolated was pneumonia in hospitalized patients (49.1%) followed by skin and skin-structure infections (19,6%), and intra-abdominal infections (18.8%). The rates of isolates with MDR, XDR, and PDX were 7.1%, 20.5%, and 0.0%. Colistin was the most active agent overall (100.0%). Amikacin was the second most active agent, inhibiting 78.9% of all isolates. Other commonly used antipseudomonal β-lactams (cefepime, ceftazidime, imipenem, meropenem, and piperacillin-tazobactam) had susceptibilities for all isolates ranging from 68.0% to 70.9%. Ciprofloxacin and levofloxacin had overall 64.0%S and 61.8%S, respectively. Ticarcillin/Clavulanic acid was the least active antimicrobial tested with overall susceptibility of 38.1%.
The results of this investigation highlight the high rates of antibiotic resistance in P. aeruginosa in the hospital which will challenge optimizing empirical antimicrobial therapy for P. aeruginosa infections and require urgent antibiotic stewardship programs effectively.
Antimicrobial, Multidrug resistance, Pseudomonas aeruginosa, Surveillance, Susceptibility
ABR: Antibiotic Resistance; ASP: Antibiotic Stewardship Programs; VNMOH: Vietnam Ministry of Health; NDGDH: Nhan Dan Gia Dinh Hospital; CLSI: Clinical Laboratory Standards Institute; SSSI: Skin-Soft Tissue Infection; MDR: Multiple Drug Resistance; XDR: Extensively Drug-Resistant; PDR: Pan Drug-Resistant; NS: Non Sensible
Antibiotic resistance (ABR) has been recognized as a global health issue. Pseudomonas aeruginosa is one of the most challenging organisms involved in a variety of infections. The World Health Organization (WHO) published a list of highly antibiotic resistant bacteria that are in need of priority for the research and development of new antibiotics. The list was divided into 3 levels, in which the most critical is the carbapenem-resistant Pseudomonas aeruginosa [1].
A geographic and temporal trend in resistant phenotypes of P. aeruginosa from ≥ 400 medical centers worldwide over the 20 years of the SENTRY Antimicrobial Surveillance Program during the period from 1997 to 2016 found that the most common infection from which P. aeruginosa was isolated was pneumonia in hospitalized patients (44.6%) followed by bloodstream infection (27.9%), with a high rate of multiple drug resistance (MDR) (27.7% vs. 23.7, respectively) [2]. Regional variations in antibiotic resistance patterns for different organisms including P. aeruginosa also occur [2], which could be due to differences in antibiotic prescribing practices. Better understanding of global trends in antibiotic resistance for the organism is obtained through local and regional surveillance studies [3].
In Vietnam, P. aeruginosa has appeared as the most commonly isolated organisms in hospitals, causing 20-30% of all nosocomial infections [4]. In 2016, the Vietnam Ministry of Health (VNMOH) approved a national program in the effort of preventing the spread of ABR and a guideline on the implementation of "Antibiotic stewardship programs (ASP) in hospitals” [5]. ASP is a multifaceted, multidisciplinary team approach to combat antibiotic misuse. Of which periodic testing and evaluation of antibiotic resistance of bacterial agents is useful for physicians to detect resistance pattern and assist in the selection of an appropriate antibiotic for empiric treatment in a particular setting.
Therefore, this study aimed to determine the status of antimicrobial resistance to anti-pseudomonal agents and the magnitude of the multi-drug resistance to P. aeruginosa in one hospital.
A retrospective review was conducted of all reports of P. aeruginosa isolates from the records of the laboratory of Nhan Dan Gia Dinh Hospital (NDGDH) between January 01, 2019 to December 31, 2019. NDGDH is a 1500-bed tertiary care referral hospital in Ho Chi Minh City, Vietnam. In cases where more than one P. aeruginosa was isolated from a single patient, the sample that is considered to be the primary source of infection is included (i.e. pulmonary excretions rather than blood in cases of pneumonia).
Submitted samples were analyzed using the traditional culture methods. Urine samples were inoculated onto blood agar and MacConkey agar. Sputum and tracheal aspirates were inoculated onto blood agar, MacConkey agar and chocolate agar. Blood samples were inoculated onto BACTEC Aerobic Plus vial, while cerebrospinal fluid and other body fluids were inoculated onto blood agar, MacConkey agar, trypticase soy broth and chocolate agar.
Identification of P. aeruginosa was based on routine biochemical methods that included the following reactions: Gram-negative bacilli, oxidase positive, unable to ferment sugars on triple sugar iron, motile, do not produce sulfide and indole, citrate positive, urease negative, lysine decarboxylase positive, lysine deaminase negative, able to grow at 42 ℃, and pigmented.
The investigated antibiotics were ticarcillin, ticarcillin/acid clavulanic, piperacillin, piperacillin/tazobactam, ceftazidime, cefepime, imipenem, meropenem, gentamicin, tobramycin, amikacin, ciprofloxacin, levofloxacin, and colistin. The in vitro susceptibility of these antibiotics was tested using the Kirby-Bauer disk diffusion method under the M02-A11 guidelines of the Clinical Laboratory Standards Institute (CLSI) and were confirmed by the automated VITEK 2 system (bioMérieux Inc., France). The subsequent results of the tests were then interpreted in accordance with the M100-S25 document.
Resistant phenotypes analysed using EUCAST criteria were as follows: MDR (NS to at least 1 antimicrobial in ≥ 3 drug classes), extensively drug-resistant ([XDR] NS to at least 1 agent in all but ≤ 2 drug classes), and pan drug-resistant (PDR), according to Magiorakos, et al. [6]. Ceftazidime-non sensible (NS) and meropenem-NS were determined according to EUCAST interpretive criteria.
P. aeruginosa, with American type culture collection (ATCC) number 27853, was used as the reference strain for quality control of culture media, biochemical tests and susceptibility testing.
The study was approved by the Nhan Dan Gia Dinh Hospital's ethical review board with approval number 15/HĐĐĐ, on 06 January 2020. The study was conducted in a spirit of respecting the private information related to patients and health care providers. Information which was collected from routine data of drug charts was anonymized.
All data was analysed by using SPSS software version 20.0. The proportion of susceptible isolates was calculated as the sum of susceptible organisms (neither intermediately susceptible nor resistant) relative to the total number of organisms tested. The drug resistance pattern of P. aeruginosa with site of infection, specific antibiotics, and resistance phenotypes was summarized in terms of frequencies and percentages.
Of 224 samples, the most common infection from which P. aeruginosa was isolated was pneumonia in hospitalized patients (49.1%) followed by skin-soft tissue infection (SSSI) (19.6%), and intra-abdominal infection (18.8%) as shown in Table 1.
Table 1: Distribution of Pseudomonas aeruginosa isolated by infection and sample type antimicrobial susceptibility. View Table 1
The rates of isolates with MDR and XDR were 7.1% and 20.5%. Pneumonia had a higher rate of isolates with MDR and XDR (11.8% and 21.8%, respectively) than BSIs (0.0% and 20.0%, respectively) as shown in Table 2. There was no PDR isolate. The frequency of XDR, ceftazidime-NS, and meropenem-NS isolates were highest in the urinary tract infection (61.1%, 76.0%, and 72.0%).
Table 2: Pseudomonas aeruginosa isolates 2019 stratified by infection type and percentage of isolates with resistant phenotypes. View Table 2
Activities of specific antimicrobials are shown in Figure 1 for all isolates and in Figure 2 for infection type. Colistin was the most active agent overall (100.0%). Amikacin was the second most active agent, inhibiting 78.9% of all isolates. Tobramycin and gentamicin were slightly less active than amikacin and inhibited 74.1% and 71.9% of all isolates, respectively. Other commonly used antipseudomonal β-lactams (cefepime, ceftazidime, imipenem, meropenem, and piperacillin-tazobactam) had susceptibilities for all isolates ranging from 68.0% to 70.9%. Ciprofloxacin and levofloxacin had overall 64.0%S and 61.8%S, respectively. Ticarcillin/Acid clavulanic was the least active antimicrobial tested with overall susceptibility of 38.1%.
 Figure 1: Susceptibilities of Pseudomonas aeruginosa (n = 224).
View Figure 1
Figure 1: Susceptibilities of Pseudomonas aeruginosa (n = 224).
View Figure 1
The resistance patterns of P. aeruginosa to the antibiotics are almost identical among infection types (Figure 2). Colistin and aminoglycosides are still the most effective as compared to other antibiotics, and ticarcillin/acid clavulanic was still noted to have the highest resistance. However, resistance of P. aeruginosa is highest in urinary tract infection, followed by BSIs.
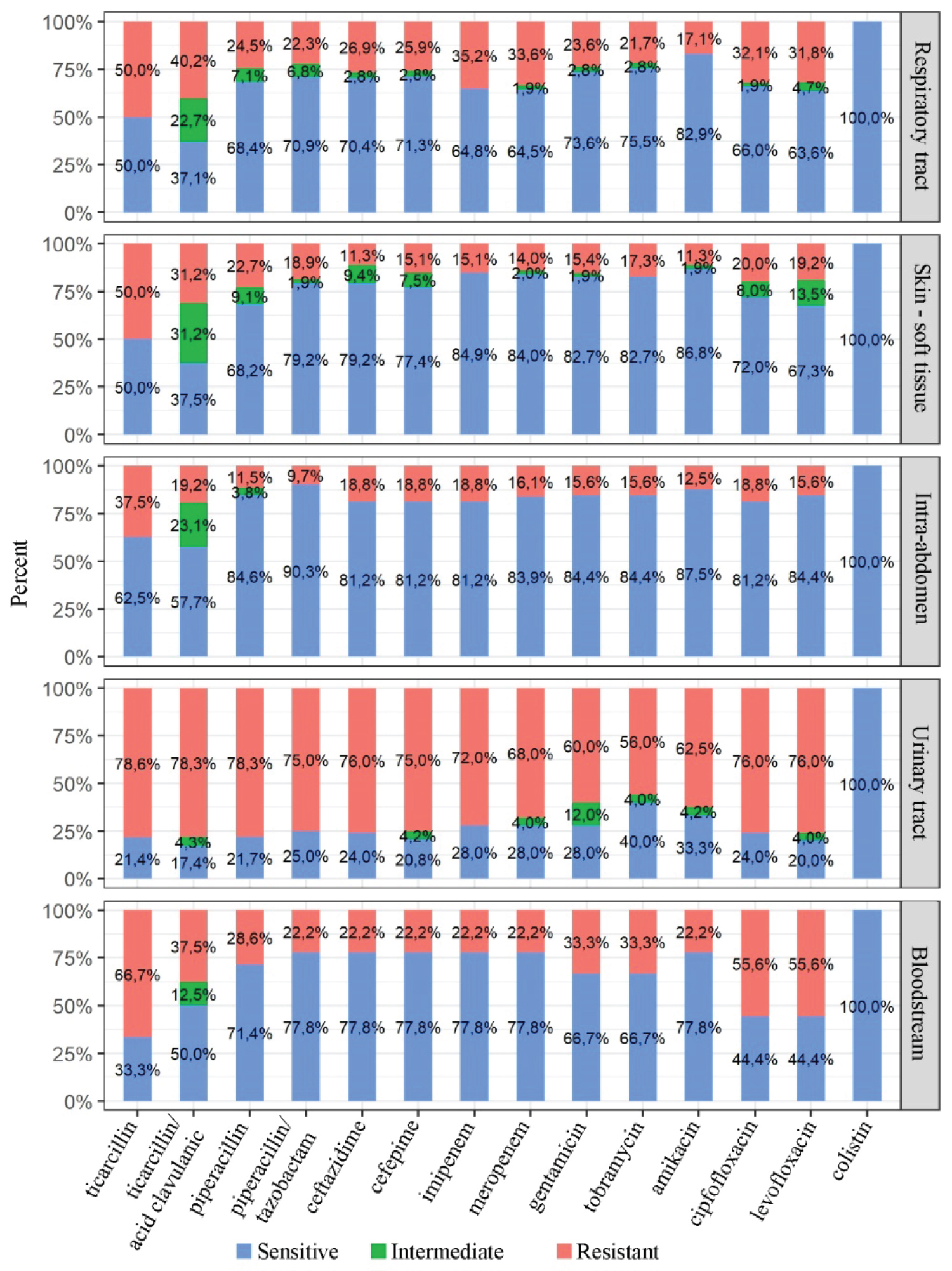 Figure 2: Susceptibilities of Pseudomonas aeruginosa for infection type (n = 224).
View Figure 2
Figure 2: Susceptibilities of Pseudomonas aeruginosa for infection type (n = 224).
View Figure 2
Resistance profile of P. aeruginosa in some studies in the literature is summarized in Table 3. Over the 20 years of SENTRY Program surveillance [2], the rates of resistant phenotypes for P. aeruginosa were highest in 2005-2008 and decreased in 2009-2016. The Asia-Pacific region had an overall lower frequency of MDR P. aeruginosa than Latin America and Europe. The region saw an increase in MDR P. aeruginosa, from 15.6% in 1997-2000 to 24.7% in 2005-2008 and decreased to 15.0% in 2013-2016. MDR P. aeruginosa in our study was lower (7.1%). XDR P. aeruginosa in 2013-2016 of SENTRY Program surveillance was 15.2% which was lower than one in our study (20.5%).
Table 3: Non-susceptibilities of Pseudomonas aeruginosa of different studies. View Table 3
The frequency of Ceftazidime-NS, and meropenem-NS isolates were one third and were highest in the urinary tract infection. A study by Biedenbach, et al. [7] found that frequency of ceftazidime-NS, and meropenem-NS P. aeruginosa from 5 medical centers in Vietnam provided 529 P. aeruginosa isolates from patients with hospital-acquired or ventilator-associated pneumonia from 2012 to 2014 was 57,7% and 43.5%, respectively.
The resistance patterns of P. aeruginosa to the antibiotics are almost identical in many studies. Colistin and aminoglycosides are still the most effective as compared to other antibiotics, followed by antipseudomonal β-lactams (cefepime, ceftazidime, imipenem, meropenem, and piperacillin-tazobactam), then quinolones. However, the rates of antibiotic -NS P. aeruginosa in our study are higher in ones in SENTRY Program surveillance.
Pneumonia had a higher rate of isolates with MDR and XDR than BSIs while the frequency of XDR, ceftazidime-NS, and meropenem-NS isolates were highest in the urinary tract infection. A study by Biedenbach, et al. [7] found that the rates of isolates NS antipseudomonal β-lactams and quinolones of Vietnamese patients with hospital-acquired or ventilator-associated pneumonia was very high and in range of 40.0%-60.0%. Similarly, carbapenem resistance was most common in Pseudomonas aeruginosa (55.7%) in Vietnamese patients in Intensive Care Units with hospital-acquired infections [8].
Compared to the results of a study by Pfaller, et al. in the period 2013-2015 [9] and Sader, et al. in the period 2012-2015 [10], our frequency of antibiotic-resistant P. aeruginosa were lower than Korea and India; and similar to Thailand; and higher than Singapore, Taiwan, Malaysia, Hong Kong, and United States.
Studies in the Asia-Pacific region have shown an increasing prevalence of metallo-β-lactamases and carbapenemases in P. aeruginosa, particularly the ST235 clone, which may explain the increase in MDR [11]. However, strain typing was not performed in this study, it is unknown whether the decrease in resistance is due to the prevalence of ST235 or other causes.
The results of this investigation highlight the high rates of antibiotic resistance in P. aeruginosa in our hospital which will challenge optimizing empirical antimicrobial therapy for P. aeruginosa infections and require urgent ASP effectively.
No.
There is no funding available for this study.
All authors don't have any conflicts of interest to declare.
Pham HT: Conceptualization, Methodology, Writing- Reviewing and Editing, Supervision; Bui QH: Data curation, Formal analysis Writing- Original draft preparation; Nguyen HH: Conceptualization, Writing- Reviewing and Editing; VoTH: Conceptualization, Methodology, Writing- Reviewing and Editing, Supervision.