The study aims to uncover the burden of brucellosis in Ghindae Zonal Referral Hospital, the therapeutic approach used at the hospital, and the outcome of treatment.
Medical records review was conducted using a data collection tool for all the brucellosis patients treated in Ghindae Zonal Referral Hospital from 2018 to 2020. Clinical finding along with Rose-Bengal test was used to diagnose 393 cases of brucellosis. Data were entered into Microsoft Excel and then exported to SPSS version 22 for analysis. Associations between variables were assessed using chi-square test and a p-value less than 0.05 was considered statistically significant.
The study showed 61% of the cases were between 15 and 60 years old with males accounting for 57.8% of the cases. About 12% suffered from anemia. The results show 7 to 10 days of therapy with gentamicin in addition to 40 to 45 days of doxycycline as a background regimen was found to be effective in more than 97% (p < 0.001). Failure and relapse rates were found to be 4.2% and 10.4% respectively.
Brucellosis was more prevalent in rural areas. A significant number of cases had anemia. The majorities were treated by a combination of doxycycline and gentamicin, and were hospitalized for one to two weeks. The above mentioned regimen was found to be effective for uncomplicated brucellosis.
Brucellosis, Zoonosis, Therapy, Diagnosis, Eritrea
Brucellosis is a zoonotic infection transmitted to humans by contact with fluids from infected animals or derived food products such as unpasteurized milk and cheese [1]. It affects people of all age groups and of both sexes. Although there has been great progress in controlling the disease in many countries, there still remain regions where the infection persists in domestic animals and, consequently, transmission to the human population frequently occurs [2]. Rose Bengal plate agglutination test is often used as a rapid screening test, with very high sensitivity (> 99%) and fairly high specificity [3]. Laboratory findings should be interpreted together with clinical manifestations, exposure history, occupation, and history of past infection [4,5]. Rose Bengal plate test is the diagnostic modality commonly used to diagnose brucellosis in Eritrea. All cases diagnosed clinically and/or by laboratory confirmation in Ghindae Zonal Referral Hospital were included in this study.
Brucellosis is an important human disease in many parts of the world, especially in the Mediterranean countries of Europe, north and east Africa, the Middle East, south and central Asia, and Central and South America and yet it is often unrecognized and frequently goes unreported. There are only a few countries in the world that are officially free of the disease [2]. Globally, an estimated 500,000 cases of brucellosis occur each year [6]. The high incidence rates of brucellosis were seen in countries such as Kenya (203.07 cases per 100,000), Yemen (89.96), Syria (47.26) and Greece (42.96) [7]. A study by McDermott & Arimi, reported 5% prevalence of brucellosis in Sub-Saharan Africa. The disease is mostly misdiagnosed and/or underreported among humans in most low and middle income countries. This is likely to contribute to spread of the disease due to limited awareness and inadequate health care infrastructure [8]. Eritrea is among the countries with highest incidence rates of human brucellosis globally, with an incidence rate of 21.82 cases per 100,000, according to Wang XH, et al. [7]. In Eritrea, most human cases appear to be related to the consumption of unpasteurized milk [9]. In cattle, the highest individual sero-prevalence was in dairy herds kept under the intensive husbandry system in Asmara, with an individual prevalence of 8.2% and unit (herd) sero-prevalence of 35.9%. This was followed by 5.0% individual sero-prevalence in the pastoral husbandry system in the Western Lowlands. The lowest was reported in the mixed crop-livestock system in the Southern Highlands with individual 0.3% and unit (village) prevalence of 2.4% [10]. According to a study conducted in 2020, the overall sero-prevalence of brucellosis in livestock owners in Foro, Afabet, Shieb, and Ghindae subzones of the Northern Red Sea Region of Eritrea was found to be 1.8% with highest in Ghindae subzone [11].
Brucellosis therapy aims to control the illness and prevent complications, relapses, and sequelae [12,13]. Brucellosis may be prevented via pasteurization or boiling of milk, vaccination of domestic livestock, serologic testing, quarantine of herds, and slaughter of infected animals. A combination of Doxycycline and Gentamicin is currently adopted as the treatment approach for most adult brucellosis patients in Eritrea. The optimal duration of Gentamicin is uncertain; but 5 days to 14 days is acceptable [14]. The minimum inhibitory concentration of Gentamicin in blood is 0.25-2 μg/ml. It is recommended to give 5 mg/kg/day of Gentamicin in 3 divided intravenous doses for 5-7 days in combination with Doxycycline as a background regimen [15]. According to the World Health Organization, it is recommended that Gentamicin be administered in a dose of 5 mg/kg/day intravenously or intramuscularly for seven to ten days in combination with Doxycycline administered for six weeks [2]. According to the Eritrean Standard Treatment Guideline, the treatment regimen for adult brucellosis in the absence to osteoarticular disease, neurobrucellosis, or endocarditis is Doxycycline 100 mg orally twice daily for 6 weeks plus streptomycin 1 gram intramuscularly once daily for the first 14 to 21 days (Gentamicin may be substituted for streptomycin) [16]. The dose and duration of Gentamicin is not clearly specified in the national guideline. Given the unavailability of streptomycin, lack of a clearly defined treatment protocol for Gentamicin compels clinicians to adopt varying therapeutic approaches. As stated in the Eritrean Standard Treatment Guideline, children less than eight years of age diagnosed with brucellosis must be treated with oral Cotrimoxazole plus Rifampicin for four to six weeks [16]. But due to the unavailability of Rifampicin, the commonly used regimen, in this case, is Cotrimoxazole plus Gentamicin. Relapse after treatment usually occurs within the first six months following completion of treatment, although it may occur up to 12 months following completion of treatment [14,17]. The research aims to study the burden of brucellosis cases in Ghindae Zonal Referral Hospital, therapeutic approaches used by clinicians at the hospital, and the outcome of treatment with the therapeutic approaches used in the hospital.
Ghindae is a town in Eritrea's Northern Red Sea Region, located 48 kilometers east of the capital. Data shows that Ghindae subzone has about 58,124 people. There are 17 administrative areas within the Ghindae subzone namely Maihabar, Nefasit, Leayten-Adiroso, Embatkala, Hutsit, Ghindae town zones 1, 2 and 3, Tseret, Agambosa, Dongolo, Gahtelay, Demas, Metkel abiet, Adi shuma, Shebah, and Fshey-Mrara. Ghindae Zonal Referral Hospital gives health services to the town of Ghindae and gets referrals from all the health institutions located in the Northern Red Sea Region.
Medical records of patients seen in Ghindae Zonal Referral Hospital were reviewed to analyze the existing burden of human brucellosis in the hospital. The study population is all the brucellosis patients diagnosed in the hospital.
Relapse: Reappearance of symptoms and signs of the disease during the 12 months after therapy.
Treatment failure: If symptoms and signs of the disease persisted or increased during or at the end of therapy.
Treated: Received the corresponding regimen in the table.
Another regimen given: Received an alternative regimen.
Not treated at all: Few cases with minor symptoms in which clear diagnosis of brucellosis or relapse could not be reached were not treated at all.
Outcome of treatment: Recorded from the clinical cards as written by the clinicians whether patient was improving or not. No laboratory or radiologic tests were used to confirm the outcome.
Improved: Condition of patient had improved upon discharge from hospital.
Not improved: Condition of patient had not improved or got worse upon discharge from hospital.
Referred: Brucellosis patient referred to National Referral Hospitals amid treatment (condition of patient is by default considered not improved).
Several factors including socio-demographic characteristics (age, sex, and address), clinical features (fever, joint pain, weight loss, unboiled milk consumption, uncooked meat consumption, prior treatment for brucellosis, family history of brucellosis, enlarged liver or spleen, lymphadenopathy, anemia, and positive Rose-Bengal test result) and therapeutic approach used (duration of gentamicin treatment, duration of doxycycline treatment, duration of cotrimoxazole treatment, improvement after treatment, and duration of stay in the hospital) were used as independent variables in the study. The outcome of treatment was used as the dependent variable.
Several factors including socio-demographic characteristics (age, sex, and address), clinical features (fever, joint pain, weight loss, unboiled milk consumption, uncooked meat consumption, prior treatment for brucellosis, family history of brucellosis, enlarged liver or spleen, lymphadenopathy, anemia, and positive Rose-Bengal test result) and therapeutic approach used (duration of gentamicin treatment, duration of doxycycline treatment, duration of cotrimoxazole treatment, improvement after treatment, and duration of stay in the hospital) were used as independent variables in the study. The outcome of treatment was used as the dependent variable.
Data collection was conducted from November 2020 to October 2021. The clinical cards of all the brucellosis patients diagnosed in Ghindae Zonal Referral Hospital in the previous three years (2018, 2019 and 2020) were traced by looking through the statistical report for inclusion in the study. The number of cases of human brucellosis included in the study was 393. It included all cases diagnosed either clinically or by laboratory confirmation and treated for uncomplicated brucellosis in Ghindae Zonal Referral Hospital. Then every brucellosis patient's clinical card was reviewed as per the questions in the checklist and recorded by data collectors who had been given an orientation on the data collection tool.
Collected data were reviewed and cleaned for any repetitions, missing information, or other errors. Then data were entered in to Microsoft Excel and then exported to SPSS version 22 which was used to analyze the existing data in terms of frequencies and percentages, and then cross-tabulation and chi-square test were used to assess associations between variables. Results with a p-value less than 0.05 were declared as statistically significant.
Ethical clearance was obtained from the Health Research Proposal Review and Ethical Committee of the Ministry of Health in Eritrea. The Northern Red Sea branch of the Ministry of Health and the administrators of Ghindae Zonal Referral Hospital were informed before commencing the study. Clinical cards of patients were reviewed by data collectors (who were treating clinicians at the hospital) and data were recorded into data collection tool that excluded names, hospital numbers, ID numbers, phone numbers or any other descriptions that could reveal the identities of the study participants. The confidentiality of participants was maintained throughout the study.
A total of 393 participants with a mean age of 22.5 (SD: 16.1) ranging from 1 to 89 years of age were enrolled in the study, 61.0% of which were 15 to 60 years of age. There were 51 children (13% of study participants) aged less than eight years. Regarding the gender of participants, 57.8% were males. Among the 393 patients included in the study, 99.5% came from the Northern Red Sea Region and only two patients came from the Central Region. A majority (92.4%) of the patients were from the Ghindae subzone. Patients coming from the rural villages of Adi shuma and Agambusa alone accounted for 31.3% of all the brucellosis cases, with Ghindae zone -3 and Hutsit each at 12.7% (Figure 1).
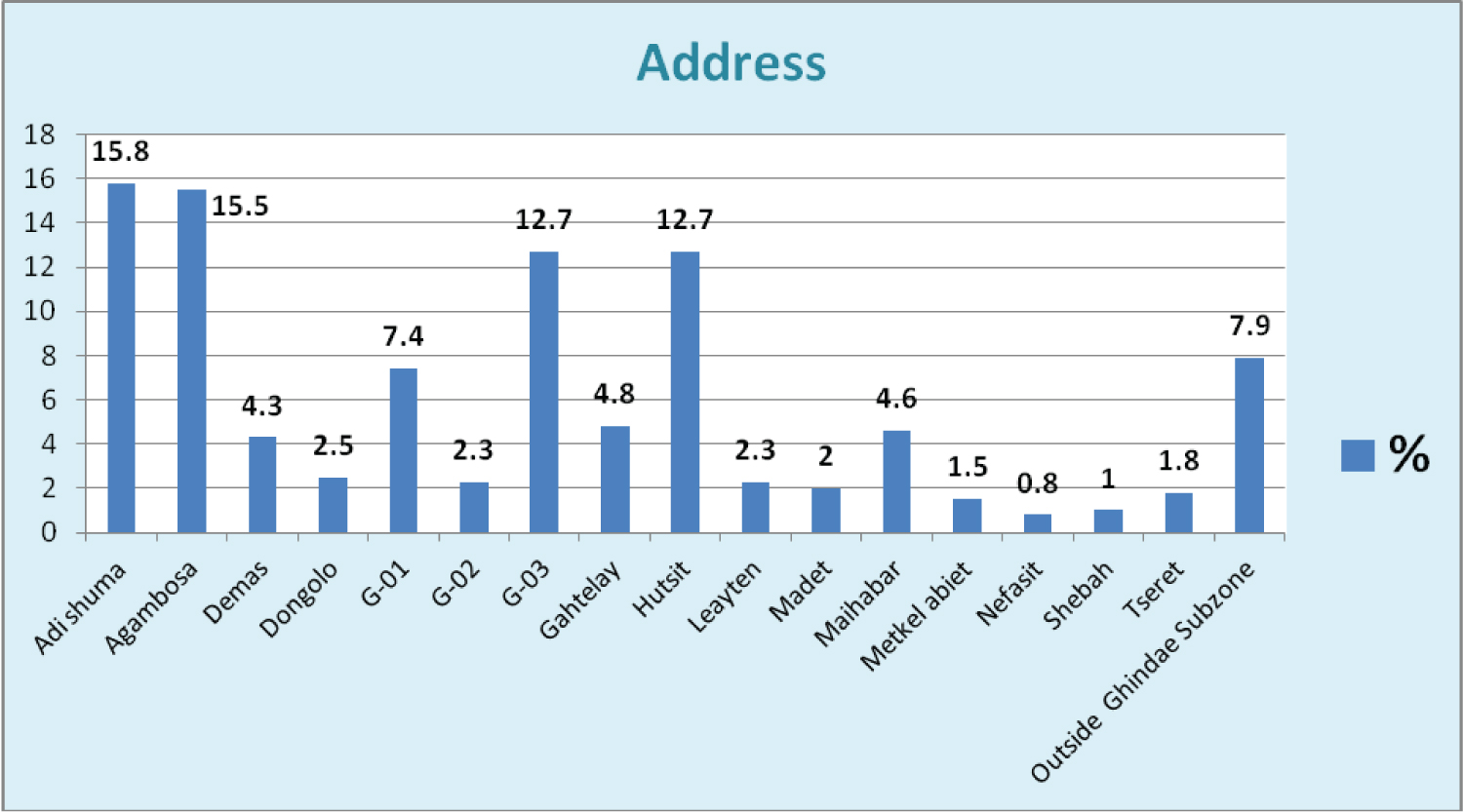 Figure 1: Addresses of the brucellosis patients included in a study conducted in 2021 in Ghindae Zonal Referral Hospital, Eritrea (n = 393).
Figure 1: Addresses of the brucellosis patients included in a study conducted in 2021 in Ghindae Zonal Referral Hospital, Eritrea (n = 393).
*G-01 = Ghindae zone 01; G-02 = Ghindae zone 02; G-03 = Ghindae zone 03
View Figure 1
Fever (94%) and joint pain (98%) were found to be among the most common presenting symptoms of brucellosis patients in the hospital. The majority (96%) of the patients diagnosed with brucellosis were found to have history of drinking unboiled milk or yogurt. History of previous diagnosis and treatment for brucellosis was reported in 10.4% of the cases suggesting the relapse rate of the disease in the area. There was a positive family history of brucellosis in 12.5% of the cases. 11.9% of cases suffered varying degrees of anemia. Rose Bengal plate test was done for 391 of the 393 cases included in the study, out of which 92.1% had positive test results (Table 1).
Table 1: Clinical features of brucellosis patients in a study conducted in 2021 in Ghindae Zonal Referral Hospital, Eritrea (n = 393). View Table 1
Data about the intake of Doxycycline plus Gentamicin was gathered for 381 patients, 85.56% of which received such therapy. Of 304 patients who received Doxycycline, 6.9% were treated for less than 40 days, while 93.1% were treated for 40 days or more. And out of 353 patients who were treated with Gentamicin, 71.4% were treated for 7-10 days, while 27.5% were treated for 11-14 days. For children less than 8 years of age, Cotrimoxazole was given instead of Doxycycline. But not all who received Cotrimoxazole were less than 8 years of age. Of the 53 children who received such treatment, 90.5% took Cotrimoxazole for duration of 40 to 45 days. Of 317 patients, 10.4% had previously been treated for brucellosis, as mentioned in table 2. Few cases with minor symptoms in which definite diagnosis of brucellosis or relapse could not be reached were not treated at all.
Table 2: Therapeutic approach used in the treatment of human brucellosis in a study conducted in 2021 in Ghindae Zonal Referral Hospital, Eritrea (n = 393). View Table 2
There was no statistically significant relationship between outcome of treatment and the age and sex of the participants. Of 222 patients who received Doxycycline plus Gentamicin, 95.5% showed improvement after treatment. However this finding was not statistically insignificant (p = 0.459). From 198 patients for whom Doxycycline was prescribed for a duration of 40 to 45 days in addition to Gentamicin, 97.5% showed improvement. Among the 178 patients who received Gentamicin treatment for 7-10 days in addition to Doxycycline as a background regimen, 97.8% showed improvement. And out of 75 patients who received Gentamicin treatment for 11-14 days in addition to Doxycycline as background regimen, 96% showed improvement after treatment. Out of 39 children less than eight years of age treated with Cotrimoxazole plus Gentamicin instead of Doxycycline plus Gentamicin, 97.3% showed improvement after starting therapy. This treatment outcome was not, however, statistically significant (p = 0.3). Out of 357 cases with available data on the hospital stay, 231 patients (64.7%) were kept in the hospital for 7-14 days, while 26.1% were treated on an outpatient basis. The remaining 6.7% were hospitalized for 1-6 days and 2.5% for over 14 days (Table 3).
Table 3: Outcome of treatment of human brucellosis in a study conducted in 2021 in Ghindae Zonal Referral Hospital, Eritrea (n = 393). View Table 3
The study showed that brucellosis was highest in people between 15 and 60 years of age probably due to higher chances of exposure to infected animals. The majority of the patients diagnosed with brucellosis in Ghindae Zonal Referral Hospital were from Ghindae subzone specifically Adishuma, Agambusa and Ghindae zone-03. Adishuma and Agambusa are villages inherently involved in rearing livestock which could be a major contributing factor. This finding was in line with a study conducted by Efrem Gebremeskel, et al. that found Ghindae Subzone with the highest sero-prevalence of brucellosis in the Northern Red Sea Region [11].
Joint pain and fever were the major complaints of the brucellosis patients coming to Ghindae Zonal Referral Hospital. Previous studies have shown that brucellosis usually consists of the insidious onset of fever, night sweats, arthralgia, myalgia, low back pain, and weight loss as well as weakness, fatigue, malaise, headache, dizziness, depression, and anorexia [15,18,19]. The majority of patients diagnosed with brucellosis claimed that they had history of consumption of unboiled or unpasteurized milk or yogurt, which is the source of infection in most instances. Anemia is a significant complication of the disease as around 12% of the patients showed varying degrees of anemia, although other causes of anemia could not be ruled out. This is consistent with the fact that anemia, leukopenia, and thrombocytopenia are the hematological signs of brucellosis according to Hofer E [20]. Most of the brucellosis patients diagnosed in Ghindae Zonal Referral Hospital received treatment after confirmation of the disease by Rose-Bengal plate test. The treatment approach used by the clinicians at the hospital is consistent with the recommendations of the WHO/CDC [2]. Positive previous history of diagnosis and treatment for brucellosis was the way of assessing the relapse rate of the disease. Other studies have shown that the rate of relapse following treatment is about 5 to 15 percent [14]. The fact that 10.4% of the brucellosis patients claimed to have previously been treated for brucellosis gives a rough picture of the relapse rate of brucellosis in Ghindae Zonal Referral Hospital. It is, however, not clear whether these are truly relapse cases or not. Rose-Bengal plate test is likely to remain positive for months after treatment. Navarro, et al. have recently shown that a significant number of successfully treated patients who remained clinically healthy for prolonged follow-up periods were still positive for Brucella DNA [21].
Patients who did not improve and those referred to higher centers after starting antibiotic treatment were classified as treatment failure. The study showed that treatment failure was 4.2%. There was no statistically significant age or gender difference in the improvement after starting antibiotic treatment. The finding in this study is consistent with studies conducted in Iran [22]. Therapeutic failures are usually associated with brucellar spondylitis and are reported in up to 15 percent of cases [23]. The majority of patients diagnosed with brucellosis were hospitalized for one to two weeks while on intravenous Gentamicin treatment. This offers light on the burden the disease is creating on the hospitals. Keeping these many patients for such durations obviously overwhelms the hospitals' limited resources, clearly implying the need for better preventive and therapeutic approaches.
The uncontrolled and retrospective nature of the study and the varying sample sizes due to documentation issues in the clinical cards were not supportive to the validity of the outcomes in the study. The source of the drugs used to treat the patients was unknown. Besides, when the clinicians wrote no abnormality detected in their physical exam findings, it was assumed that there was no anemia, no organomegally and no lymphadenopathy. There was also loss to follow patients and difficulty in measuring outcome of the given treatments. The chosen hospital may not fully represent the region or the country. Patients who did not improve with therapy and those referred to National Referral Hospitals could have had certain super-imposed pathologies that could not have been ruled out in Ghindae Zonal Referral Hospital considering the shortage of diagnostic modalities in the hospital.
In the current study, brucellosis was seen to be more prevalent in rural areas where people are involved in rearing livestock. Anemia was seen to be a common complication of the disease. Despite the acceptable success rate of the treatment approach followed in Ghindae Zonal Referral Hospital, significant variation in treatment strategies was observed among different clinicians at the hospital. Treating patients with uncomplicated brucellosis with Doxycycline as a background regimen for 40-45 days along with Gentamicin injections for 7-10 days was found to be effective, although a broader prospective study or clinical trial is recommended. Considering the significant burden of the disease, a clearly defined national guideline for the treatment (with available drugs) and prevention of brucellosis should be disseminated to all the hospitals in the country.
ETM and DK contributed to study concept, design, drafting of manuscript, and acquisition of data. All authors were involved in the analysis and interpretation of data. FK and ETM performed the statistical analysis. ETM supervised the study. All authors read, critically reviewed, and approved the final manuscript.
This study was partially funded by the Northern Red Sea zonal division of the Ministry of Health, Eritrea. The funder did not take any role in the design, conduct, analysis, interpretation of data, writing the report, or in the decision to submit the article for publication.
The authors declared that they had no conflicts of interest.
The authors sincerely thank the Northern Red Sea zonal division of the Ministry of Health for their continued motivation and acknowledge the data collectors and patients who took part in the study.
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.