

Journal of Dermatology Research and Therapy
Esophagitis Dissecans Superficialis with Concomitant Bullous Pemphigoid: A Case Report
Shawn L Shah1*, Joan Paul2, Alicia T Dagrosa3, Erik Jenson4, Zilla Hussain1, Stuart Gordon1 and Michael Shane Chapman2
1Division of Gastroenterology and Hepatology, Dartmouth-Hitchcock Medical Center, Lebanon, New Hampshire, USA
2Division of Surgery, Section of Dermatology, Dartmouth-Hitchcock Medical Center, Lebanon, New Hampshire, USA
3Geisel School of Medicine at Dartmouth, Lebanon, New Hampshire, USA
4Division of Pathology, Dartmouth-Hitchcock Medical Center, Lebanon, New Hampshire, USA
*Corresponding author:
Shawn L Shah, Division of Gastroenterology and Hepatology, Dartmouth-Hitchcock Medical Center, Lebanon, New Hampshire, USA, Tel: 603-650-7515, E-mail: ShawnLShah@gmail.com
J Dermatol Res Ther, JDRT-2-029, (Volume 2, Issue 4), Case Report; ISSN: 2469-5750
Received: May 29, 2016 | Accepted: July 15, 2016 | Published: July 18, 2016
Citation: Shah SL, Paul J, Dagrosa AT, Jenson E, Hussain Z, et al. (2016) Esophagitis Dissecans Superficialis with Concomitant Bullous Pemphigoid: A Case Report. J Dermatol Res Ther 2:029. 10.23937/2469-5750/1510029
Copyright: © 2016 Shah SL, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Esophagitis dissecans superficialis (EDS) is a rare endoscopic finding characterized by sloughing of the esophageal mucosal lining, which has been infrequently associated with autoimmune bullous dermatoses. We report a case of a 77-year-old man who presented with diffuse mucocutaneous bullous lesions and odynophagia. Direct immunofluorescence of a skin biopsy confirmed a diagnosis of bullous pemphigoid and esophagogastroduodenoscopy revealed linear fissures and sloughing of the esophageal mucosa consistent with a diagnosis of EDS. With only two previously reported cases of EDS associated with bullous pemphigoid, prompt endoscopic evaluation should be considered in patients with bullous lesions and gastrointestinal symptoms.
Abbreviations
BP: Bullous Pemphigoid; C3: Complement 3; EDS: Esophagitis Dissecans Superficialis; Igg: Immunoglobulin G; MMP: Mucous Membrane Pemphigoid; PPI: Proton Pump Inhibitor
Introduction
Esophagitis dissecans superficialis (EDS) is an exceedingly rare endoscopic finding that is characterized by sloughing of the esophageal mucosal lining [1]. First described by Rosenberg in the late 1800s, EDS can be visualized endoscopically as stripped off or denuded mucosa, vertical fissures, linear furrows or circumferential cracks along the esophagus [2,3]. The clinical presentation tends to be variable, ranging from an absence of symptoms to chest discomfort, dysphagia, odynophagia, and reflux [4,5]. While the clinical significance of EDS is poorly understood, the etiologies associated with the finding are rather diverse and include medications, such as bisphosphonates and nonsteroidal anti-inflammatory drugs, chemical irritants, celiac disease, collagen vascular disease and autoimmune bullous dermatoses [1,2,6,7]. Interestingly, esophageal involvement in vesiculobullous dermatoses is rather uncommon with most reported cases being associated with pemphigus vulgaris and mucus membrane pemphigoid (MMP) [5]. Here we present an unusual case of EDS associated with bullous pemphigoid (BP).
Case
A 77-year-old man with essential hypertension and morbid obesity presented with a 2-month history of diffuse mucocutaneous bullous lesions with recent onset of odynophagia and melenic stools that had developed over the week prior to admission. Pertinent home medications included losartan-hydrochlorothiazide, propranolol, and levothyroxine. He reported pruritic blisters that had spread from his wrists to his upper and lower extremities with concomitant involvement of the oral cavity. The patient had presented to an outside emergency department twice during this 2-month period and was empirically treated with a 5-day course of oral prednisone (60 mg daily) each time with nominal improvement.
Upon presentation to our institution, the patient was afebrile with a normal heart rate but with evidence of orthostatic hypotension. Physical exam findings were notable for tense bullae along the wrists and ankles, edematous urticarial papules and plaques with overlying hemorrhagic crust along the abdomen and upper and lower extremities encompassing approximately 30% of the body surface area, superficial erosions along the upper and lower extremities covering approximately 5% of the body surface area, and punctate erosions along the inside of the lower lip and tongue (Figure 1). The patient's face, back, and genitalia had no pertinent dermatologic findings. Nikolsky and Asboe-Hansen signs were both negative. Laboratory data were notable for a neutrophilic leukocytosis (12,800 cells per microliter), a peripheral eosinophilia (1,600 cells per microliter) and a normocytic anemia with a hemoglobin of 8.8 grams per deciliter.

.
Figure 1: Bullous Pemphigoid (BP). Edematous urticarial papules and plaques with overlying hemorrhagic crust along the left wrist and volar forearm, as well as denuded bullae along the left knee and lower leg.
View Figure 1
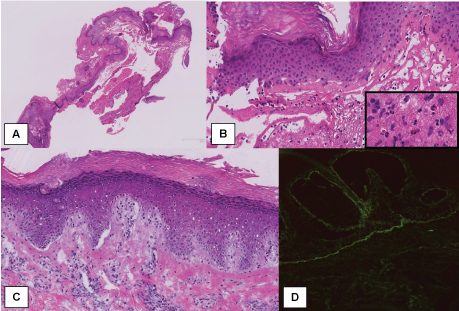
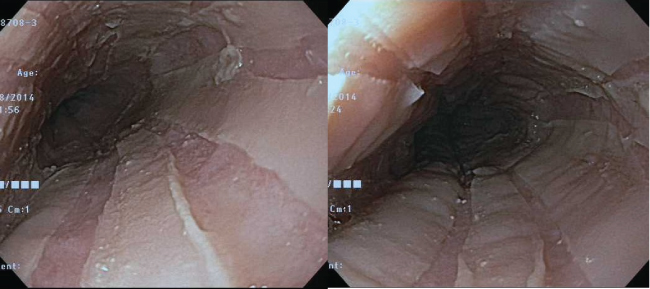
A biopsy of the perilesional skin under direct immunofluorescence demonstrated linear immunoglobulin G (IgG) and complement 3 (C3) deposition at the dermoepidermal junction (Figure 2: Panel D). Additionally, a hematoxylin and eosin-stained sample from an intact bulla on the left volar wrist revealed a subepidermal blister with an eosinophilic infiltrate in the upper dermis (Figure 2: Panel A, Panel B and Panel C). The histopathological findings confirmed a diagnosis of BP. Given the patient's continued melena, an esophagogastroduodenoscopy was performed, which revealed vertical linear fissures with sloughing of the superficial esophageal mucosa from the proximal to distal esophagus, suggestive of EDS (Figure 3). An esophageal biopsy was deferred given the friability of the mucosa and risk of bleeding. In addition to continuing treatment with a proton pump inhibitor (PPI), the patient was started on intravenous methylprednisolone (1 gram per day for 3 days) along with topical triamcinolone 0.1% ointment. On day 4, he was started on an oral prednisone taper (60 mg for 5 days followed by 40 mg for 5 days, then 20 mg for 5 days, and then 10 mg for 5 days). The patient was discharged on hospital day 8 with complete resolution of his odynophagia and melenic stools, as well as marked improvement of his bullous mucocutaneous lesions. He was sent home with instructions to complete the aforementioned oral prednisone taper and continue the PPI. The patient was started on mycophenolate mofetil (500 mg twice daily) as an outpatient and achieved full resolution of his mucocutaneous lesions. A repeat endoscopy was declined by the patient with no further episodes of odynophagia or melenic stools.
.
Figure 2: Bullous Pemphigoid (BP). Lesional and perilesional skin punch biopsies (Panels A-C: Hematoxylin and Eosin stain; Panel D: Direct immunofluorescence for IgG). Subepidermal blistering with separation of the viable epidermal blister roof from the underlying dermis is identified on a lesional punch biopsy (Panel A). A higher-power view (Panel B) shows a cellular infiltrate consisting of neutrophils and eosinophils (inset). A perilesional punch biopsy (Panel C) demonstrates subepidermal clefts representing early bullae; note the spongiosis and perivascular lymphocytes (lower aspect of the image). Direct immunofluorescence of the perilesional skin (Panel D) reveals linear IgG deposition along the basement membrane zone. Direct immunofluorescence of C3 (not pictured) also showed linear staining along the basement membrane.
View Figure 2
.
Figure 3: Esophagitis Dissecans Superficialis (EDS). An endoscopic view of EDS. Note the vertical linear fissures with extensive sloughing of the superficial esophageal mucosa extending from the proximal to the distal esophagus.
View Figure 3
Discussion
The esophageal squamous epithelium consists of a dynamic cell population that is incessantly renewed; however, complete denuding of the esophageal mucosal is described as an entity known as esophagitis dissecans superficialis (EDS). EDS is primarily an endoscopic finding with no existing diagnostic criteria, although histopathologic features include marked parakeratosis and orthokeratosis, desquamation of the squamous layer, and epithelial inflammation and necrosis [1]. Carmack et al. noted in their clinicopathological study of 12 cases of EDS that the aforementioned histological features often overlap with other esophageal diseases, making the clinical presentation vital in lending credence to a diagnosis of EDS [1]. Furthermore, characteristic histologic features of EDS, such as suprabasal acantholysis, are routinely not identified with esophageal biopsies, as samples do not typically include the basement membrane secondary to the tangential position of the endoscope and forceps inside the esophagus [5,7,8]. Hokama et al. reported that perhaps enzyme-linked immunosorbent assay of these samples could be used to detect characteristic antibodies in a simpler and more quantifiable manner than immunofluorescence, with the latter being useful for monitoring disease activity [7].
Bullous pemphigoid is an uncommon autoimmune immunobullous disorder that characteristically affects patients over the age of 60 [9]. Pathogenesis of BP involves tissue-bound and circulating autoantibodies directed against BP antigen 180 (BP180, BPAG2, or type XVII collagen) and BP antigen 230 (BP230 or BPAG1). Autoreactive T-cells then respond to BP180 and BP230 by stimulating B-cells to produce autoantibodies and promote tissue damage via helper T-cell cytokines. Diagnostically, fine linear deposition of IgG4, IgG1 and/or C3 along the epidermal basement membrane is seen on direct immunofluorescence studies of uninvolved perilesional skin. A subepidermal blister along with eosinophilic infiltrate in the upper dermis is typically seen on light microscopy. Classically, patients with BP present with pruritic vesicles and bullae on either normal or erythematous skin, as well as urticarial papules and plaques on the flexural extremities and trunk. Ten to thirty percent of patients with BP may also have oral involvement, but esophageal involvement has rarely been reported.
Foroozan et al. reported the first case of EDS associated with mucous membrane pemphigoid (MMP) in 1967 [10]. Mucous membrane pemphigoid, or cicatricial pemphigoid, is a rare autoimmune bullous disease related to, but distinct from BP. Mucous membrane pemphigoid characteristically affects the oral and ocular mucosa with infrequent skin involvement, and is treated with dapsone rather than systemic corticosteroids as the mainstay of therapy [9] Esophageal involvement occurs in 4-8% of patients with MMP and typically involves mucosal erosions, webs, and strictures of the cervical esophagus, but rarely EDS [7,11,12]. In contrast, esophageal involvement has been infrequently reported with BP, while being more commonly cited with pemphigus vulgaris [7]. As previously mentioned, a diagnosis of BP via esophageal biopsy can be rather challenging for a variety of reasons. However, Galloro and colleagues argue that a successful biopsy can be safely achieved with a rocking biopsy forceps, as demonstrated in a study of 16 patients with immunobullous disease [8]. Indeed, in a case series of 28 patients with oral pemphigus vulgaris, no endoscopy-related complications manipulating the esophageal lesions were reported [4]. However, larger studies must be conducted as many consider endoscopic biopsies of such lesions to be risky given the extreme fragility of the esophageal mucosa with potential to aggravate existing lesions [13]. Nonetheless, since upper endoscopy represents the definitive diagnostic tool to evaluate the esophageal mucosa and collect biopsies for histopathologic studies, Galloro et al. recommend that its use be routine among patients with immunobullous disorders with concomitant esophageal complaints [4].
To date, there have been only two reported cases of EDS associated with BP (Table 1) [5,14]. Esophageal bullae or erosions have been reported with BP, but EDS or sloughing esophagus is an underreported and under-recognized entity [15-21].
![]()
Table 1: Two reported cases of esophagitis dissecans superficialis associated with bullous pemphigoid.
View Table 1
Our patient experienced complete remission of his mucocutaneous lesions with systemic steroids and mycophenolate mofetil; however, he declined repeat endoscopy after his skin lesions resolved. Interestingly, the natural course of EDS appears benign despite its often impressive appearance under endoscopy. Most cases completely resolve after treatment of the underlying condition (e.g., autoimmune bullous dermatoses) in combination with a PPI [22]. However, since esophageal involvement can persist despite apparent clearance of skin lesions whilst on immunosuppressive therapy, EDS should be on the differential for patients presenting with melena and a history of an autoimmune blistering disorder [5]. Esophageal lesions can also be the presenting sign of bullous dermatoses, sometimes occurring months to years before the onset of the characteristic cutaneous lesions of BP or pemphigus vulgaris [23]. While only two prior cases of EDS associated with BP have been described in the English literature, prompt endoscopic evaluation should be considered among patients with bullous lesions and associated gastrointestinal symptoms.
References
-
Carmack SW, Vemulapalli R, Spechler SJ, Genta RM (2009) Esophagitis dissecans superficialis ("sloughing esophagitis"): a clinicopathologic study of 12 cases. Am J Surg Pathol 33: 1789-1794.
-
Brandt L (2011) Esophagitis dissecans superficialis. Gastrointest Endosc 74: 403-404.
-
Rosenberg B (1892) Oesophagitis dissecans superficialis. Centralbl Allg Pathol u path Anat 3: 753-759.
-
Galloro G, Mignogna M, de Werra C, Magno L, Diamantis G, et al. (2005) The role of upper endoscopy in identifying oesophageal involvement in patients with oral pemphigus vulgaris. Dig Liver Dis 37: 195-199.
-
Tijjani BM, Masoodi I, Hassan SN (2013) Esophagitis dissecans superficialis presenting with massive haematemesis in a patient with bullous pemphigoid. Niger J Med 22: 354-356.
-
Hage-Nassar G, Rotterdam H, Frank D, Green PH (2003) Esophagitis dissecans superficialis associated with celiac disease. Gastrointest Endosc 57: 140-141.
-
Akira Hokama, Yu-ichi Yamamoto, Kiyohito Taira, Mitsuteru Nakamura, Chiharu Kobashigawa, et al. (2010) Esophagitis dissecans superficialis and autoimmune bullous dermatoses: a review. World J Gastrointest Endosc 2: 252-256.
-
Galloro G, Diamantis G, Magno L, Inzirillo M, Mignogna MC, et al. (2007) Technical aspects in endoscopic biopsy of lesions in esophageal pemphigus vulgaris. Dig Liver Dis 39: 363-367.
-
Bolognia JL, Jorizzo JL, Schaffer JV (2012) Dermatology. (3rd edn), Elsevier Saunders, 475-487.
-
Foroozan P, Enta T, Winship DH, Trier JS (1967) Loss and regeneration of the esophageal mucosa in pemphigoid. Gastroenterology 52: 548-558.
-
Wise JL, Murray JA (2002) Esophageal Manifestations of Dermatologic Disease. Current Gastroenterology Reports 4: 205-212.
-
Sallout H, Anhalt GJ, Al-Kawas FH (2000) Mucous membrane pemphigoid presenting with isolated esophageal involvement: a case report. Gastrointest Endosc 52: 429-433.
-
Revuz J (2000) Oesophageal involvement in pemphigus vulgaris. Lancet 355: 656.
-
Mönkemüller K, Neumann H, Fry LC (2010) Esophageal blebs and blisters. Gastroenterology 138: e3-4.
-
Akhondi H (2014) Sloughing esophagitis: a not so common entity. Int J Biomed Sci 10: 282-286.
-
Chong VH, Lim CC, Vu C (2006) A rare cause of acute upper gastrointestinal bleeding. Surg Laparosc Endosc Percutan Tech 16: 91-93.
-
Eng TY, Hogan WJ, Jordon RE (1978) Oesophageal involvement in bullous pemphigoid. A possible cause of gastrointestinal haemorrhage. Br J Dermatol 99: 207-214.
-
Maharshak N, Sagi M, Santos E, Sprecher E, Goldberg I (2013) Oesophageal involvement in bullous pemphigoid. Clin Exp Dermatol 38: 274-275.
-
Nagashima R, Tsuge K, Harada M, Katagiri Y, Shinzawa H, et al. (2000) Endoscopic hemostasis of hemorrhage from esophageal bullous pemphigoid. Gastrointest Endosc 52: 433-434.
-
Sharon P, Greene ML, Rachmilewitz D (1978) Esophageal involvement in bullous emphigoid. Gastrointest Endosc 24: 122-123.
-
Tabuchi K, Nomura M, Murashita H, Fujisawa Y, Tsuji S, et al. (2006) Coexistence of pemphigus vulgaris and bullous pemphigoid in the upper aerodigestive tract. Auris Nasus Larynx 33: 231-233.
-
Albert DM, Ally MR, Moawad FJ (2013) The sloughing esophagus: a report of five cases. Am J Gastroenterol 108: 1816-1817.
-
Raque CJ, Stein KM, Samitz MH (1970) Pemphigus vulgaris involving the esophagus. Arch Dermatol 102: 371-373.
